

Pharmacokinetics-pharmacodynamics issues relevant for the clinical use of beta-lactam antibiotics in critically ill patients
- PMID: 30244674
- PMCID: PMC6151903
- DOI: 10.1186/s13054-018-2155-1
Pharmacokinetics-pharmacodynamics issues relevant for the clinical use of beta-lactam antibiotics in critically ill patients
Abstract
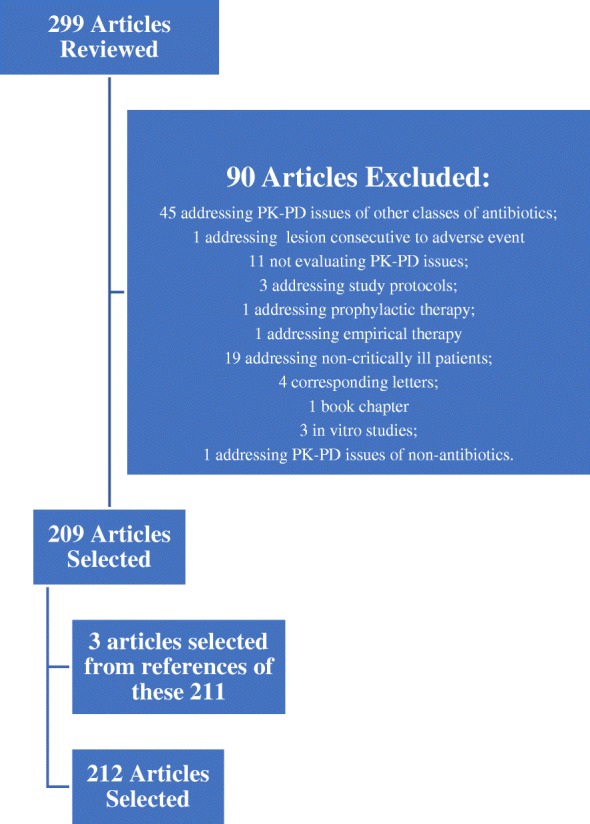
Antimicrobials are among the most important and commonly prescribed drugs in the management of critically ill patients and beta-lactams are the most common antibiotic class used. Critically ill patient's pathophysiological factors lead to altered pharmacokinetics and pharmacodynamics of beta-lactams.A comprehensive bibliographic search in PubMed database of all English language articles published from January 2000 to December 2017 was performed, allowing the selection of articles addressing the pharmacokinetics or pharmacodynamics of beta-lactam antibiotics in critically ill patients.In critically ill patients, several factors may increase volume of distribution and enhance renal clearance, inducing high intra- and inter-patient variability in beta-lactam concentration and promoting the risk of antibiotic underdosing. The duration of infusion of beta-lactams has been shown to influence the fT > minimal inhibitory concentration and an improved beta-lactam pharmacodynamics profile may be obtained by longer exposure with more frequent dosing, extended infusions, or continuous infusions.The use of extracorporeal support techniques in the critically ill may further contribute to this problem and we recommend not reducing standard antibiotic dosage since no drug accumulation was found in the available literature and to maintain continuous or prolonged infusion, especially for the treatment of infections caused by multidrug-resistant bacteria.Prediction of outcome based on concentrations in plasma results in overestimation of antimicrobial activity at the site of infection, namely in cerebrospinal fluid and the lung. Therefore, although no studies have assessed clinical outcome, we recommend using higher than standard dosing, preferably with continuous or prolonged infusions, especially when treating less susceptible bacterial strains at these sites, as the pharmacodynamics profile may improve with no apparent increase in toxicity.A therapeutic drug monitoring-guided approach could be particularly useful in critically ill patients in whom achieving target concentrations is more difficult, such as obese patients, immunocompromised patients, those infected by highly resistant bacterial strains, patients with augmented renal clearance, and those undergoing extracorporeal support techniques.
Keywords: Antibiotics; Critical care or intensive care or critically ill; Pharmacodynamics; Pharmacokinetics; Sepsis or septic shock.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Puskarich MA, Trzeciak S, Shapiro NI, Arnold RC, Horton JM, Studnek JR, Kline JA, Jones AE, On behalf of the Emergency Medicine Shock Research Network Association between timing of antibiotic administration and mortality from septic shock in patients treated with a quantitative resuscitation protocol. Crit Care Med. 2011;39:2066–2071. doi: 10.1097/CCM.0b013e31821e87ab. - DOI - PMC - PubMed
-
- Kumar A, Roberts D, Wood KE, Light B, Parrillo JE, Sharma S, Suppes R, Feinstein D, Zanotti S, Taiberg L, Gurka D, Kumar A, Cheang M. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med. 2006;34:1589–1596. doi: 10.1097/01.CCM.0000217961.75225.E9. - DOI - PubMed
-
- Roberts J. A., Paul S. K., Akova M., Bassetti M., De Waele J. J., Dimopoulos G., Kaukonen K.-M., Koulenti D., Martin C., Montravers P., Rello J., Rhodes A., Starr T., Wallis S. C., Lipman J., Roberts J. A., Lipman J., Starr T., Wallis S. C., Paul S. K., Margarit Ribas A., De Waele J. J., De Crop L., Spapen H., Wauters J., Dugernier T., Jorens P., Dapper I., De Backer D., Taccone F. S., Rello J., Ruano L., Afonso E., Alvarez-Lerma F., Gracia-Arnillas M. P., Fernandez F., Feijoo N., Bardolet N., Rovira A., Garro P., Colon D., Castillo C., Fernado J., Lopez M. J., Fernandez J. L., Arribas A. M., Teja J. L., Ots E., Carlos Montejo J., Catalan M., Prieto I., Gonzalo G., Galvan B., Blasco M. A., Meyer E., Del Nogal F., Vidaur L., Sebastian R., Garde P. M., Martin Velasco M. d. M., Zaragoza Crespo R., Esperatti M., Torres A., Montravers P., Baldesi O., Dupont H., Mahjoub Y., Lasocki S., Constantin J. M., Payen J. F., Martin C., Albanese J., Malledant Y., Pottecher J., Lefrant J.-Y., Jaber S., Joannes-Boyau O., Orban C., Ostermann M., McKenzie C., Berry W., Smith J., Lei K., Rubulotta F., Gordon A., Brett S., Stotz M., Templeton M., Rhodes A., Ebm C., Moran C., Kaukonen K.-M., Pettila V., Dimopoulos G., Koulenti D., Xristodoulou A., Theodorou V., Kouliatsis G., Sertaridou E., Anthopoulos G., Choutas G., Rantis T., Karatzas S., Balla M., Papanikolaou M., Myrianthefs P., Gavala A., Fildisis G., Koutsoukou A., Kyriakopoulou M., Petrochilou K., Kompoti M., Michalia M., Clouva-Molyvdas F.-M., Gkiokas G., Nikolakopoulos F., Psychogiou V., Malliotakis P., Akoumianaki E., Lilitsis E., Koulouras V., Nakos G., Kalogirou M., Komnos A., Zafeiridis T., Chaintoutis C., Arvaniti K., Matamis D., Chaintoutis C., Kydona C., Gritsi-Gerogianni N., Giasnetsova T., Giannakou M., Soultati I., Chytas I., Antoniadou E., Antipa E., Lathyris D., Koukoubani T., Paraforou T., Spiropoulou K., Bekos V., Spring A., Kalatzi T., Nikolaou H., Laskou M., Strouvalis I., Aloizos S., Kapogiannis S., Soldatou O., Bassetti M., Adembri C., Villa G., Giarratano A., Maurizio Raineri S., Cortegiani A., Montalto F., Strano M. T., Ranieri V. M., Sandroni C., De Pascale G., Molin A., Pelosi P., Montagnani L., Urbino R., Mastromauro I., De Rosa F. G., Ranieri V. M., Cardoso T., Afonso S., Goncalves-Pereira J., Baptista J. P., Akova M., Ozveren A. DALI: Defining Antibiotic Levels in Intensive Care Unit Patients: Are Current -Lactam Antibiotic Doses Sufficient for Critically Ill Patients? Clinical Infectious Diseases. 2014;58(8):1072–1083. doi: 10.1093/cid/ciu027. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
