

Net ultrafiltration intensity and mortality in critically ill patients with fluid overload
- PMID: 30244678
- PMCID: PMC6151928
- DOI: 10.1186/s13054-018-2163-1
Net ultrafiltration intensity and mortality in critically ill patients with fluid overload
Abstract
Background: Although net ultrafiltration (UFNET) is frequently used for treatment of fluid overload in critically ill patients with acute kidney injury, the optimal intensity of UFNET is unclear. Among critically ill patients with fluid overload receiving renal replacement therapy (RRT), we examined the association between UFNET intensity and risk-adjusted 1-year mortality.
Methods: We selected patients with fluid overload ≥ 5% of body weight prior to initiation of RRT from a large academic medical center ICU dataset. UFNET intensity was calculated as the net volume of fluid ultrafiltered per day from initiation of either continuous or intermittent RRT until the end of ICU stay adjusted for patient hospital admission body weight. We stratified UFNET as low (≤ 20 ml/kg/day), moderate (> 20 to ≤ 25 ml/kg/day) or high (> 25 ml/kg/day) intensity. We adjusted for age, sex, body mass index, race, surgery, baseline estimated glomerular filtration rate, oliguria, first RRT modality, pre-RRT fluid balance, duration of RRT, time to RRT initiation from ICU admission, APACHE III score, mechanical ventilation use, suspected sepsis, mean arterial pressure on day 1 of RRT, cumulative fluid balance during RRT and cumulative vasopressor dose during RRT. We fitted logistic regression for 1-year mortality, Gray's survival model and propensity matching to account for indication bias.
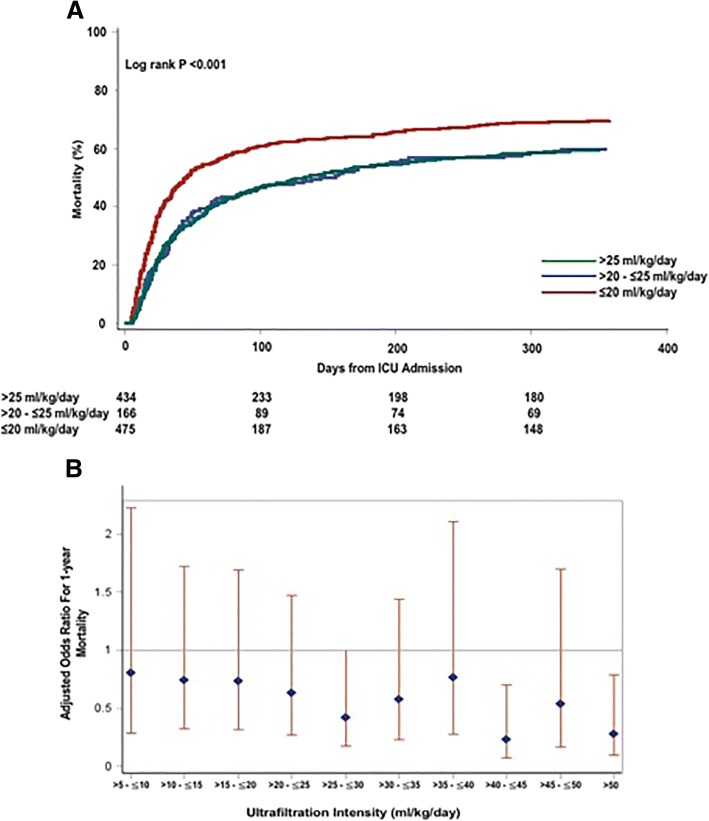
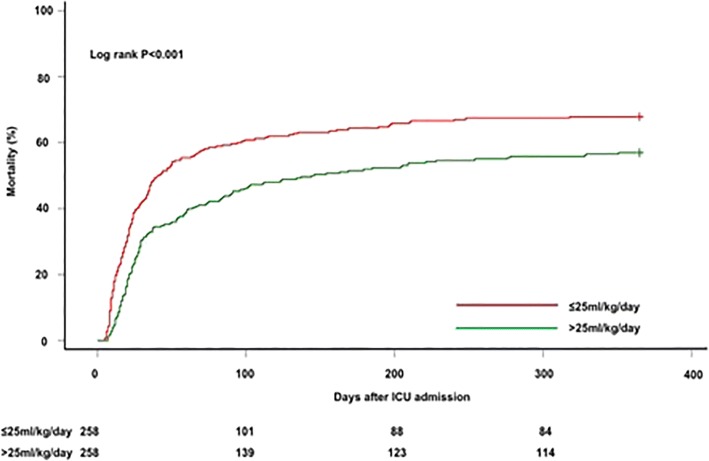
Results: Of 1075 patients, the distribution of high, moderate and low-intensity UFNET groups was 40.4%, 15.2% and 44.2% and 1-year mortality was 59.4% vs 60.2% vs 69.7%, respectively (p = 0.003). Using logistic regression, high-intensity compared with low-intensity UFNET was associated with lower mortality (adjusted odds ratio 0.61, 95% CI 0.41-0.93, p = 0.02). Using Gray's model, high UFNET was associated with decreased mortality up to 39 days after ICU admission (adjusted hazard ratio range 0.50-0.73). After combining low and moderate-intensity UFNET groups (n = 258) and propensity matching with the high-intensity group (n = 258), UFNET intensity > 25 ml/kg/day compared with ≤ 25 ml/kg/day was associated with lower mortality (57% vs 67.8%, p = 0.01). Findings were robust to several sensitivity analyses.
Conclusions: Among critically ill patients with ≥ 5% fluid overload and receiving RRT, UFNET intensity > 25 ml/kg/day compared with ≤ 20 ml/kg/day was associated with lower 1-year risk-adjusted mortality. Whether tolerating intensive UFNET is just a marker for recovery or a mediator requires further research.
Keywords: Dialysis; Fluid overload; Intensity; Mortality; Net ultrafiltration; Renal replacement therapy.
Conflict of interest statement
Ethics approval and consent to participate
This project was approved by the University of Pittsburgh Institutional Review Board.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Comment in
-
How to understand real net ultrafiltration and its association with low blood pressure in critically ill patients with renal replacement therapy.Crit Care. 2019 Jan 23;23(1):20. doi: 10.1186/s13054-018-2298-0. Crit Care. 2019. PMID: 30674339 Free PMC article.
References
-
- Bellomo R, Cass A, Cole L, Finfer S, Gallagher M, Lee J, Lo S, McArthur C, McGuiness S, et al. An observational study fluid balance and patient outcomes in the randomized evaluation of normal vs. augmented level of replacement therapy trial. Crit Care Med. 2012;40(6):1753–1760. doi: 10.1097/CCM.0b013e318246b9c6. - DOI - PubMed
-
- Vaara ST, Korhonen AM, Kaukonen KM, Nisula S, Inkinen O, Hoppu S, Laurila JJ, Mildh L, Reinikainen M, Lund V, et al. Fluid overload is associated with an increased risk for 90-day mortality in critically ill patients with renal replacement therapy: data from the prospective FINNAKI study. Crit Care. 2012;16(5):R197. doi: 10.1186/cc11682. - DOI - PMC - PubMed
-
- Bouchard J, Soroko SB, Chertow GM, Himmelfarb J, Ikizler TA, Paganini EP, Mehta RL, Program to Improve Care in Acute Renal Disease Study Group Fluid accumulation, survival and recovery of kidney function in critically ill patients with acute kidney injury. Kidney Int. 2009;76(4):422–427. doi: 10.1038/ki.2009.159. - DOI - PubMed
-
- KDIGO Clinical practice guideline for acute kidney injury. Kidney Int Suppl. 2012;2:1–138. doi: 10.1038/kisup.2012.1. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
