

Neurological complications of immune checkpoint inhibitors: what happens when you 'take the brakes off' the immune system
- PMID: 30245744
- PMCID: PMC6144585
- DOI: 10.1177/1756286418799864
Neurological complications of immune checkpoint inhibitors: what happens when you 'take the brakes off' the immune system
Abstract
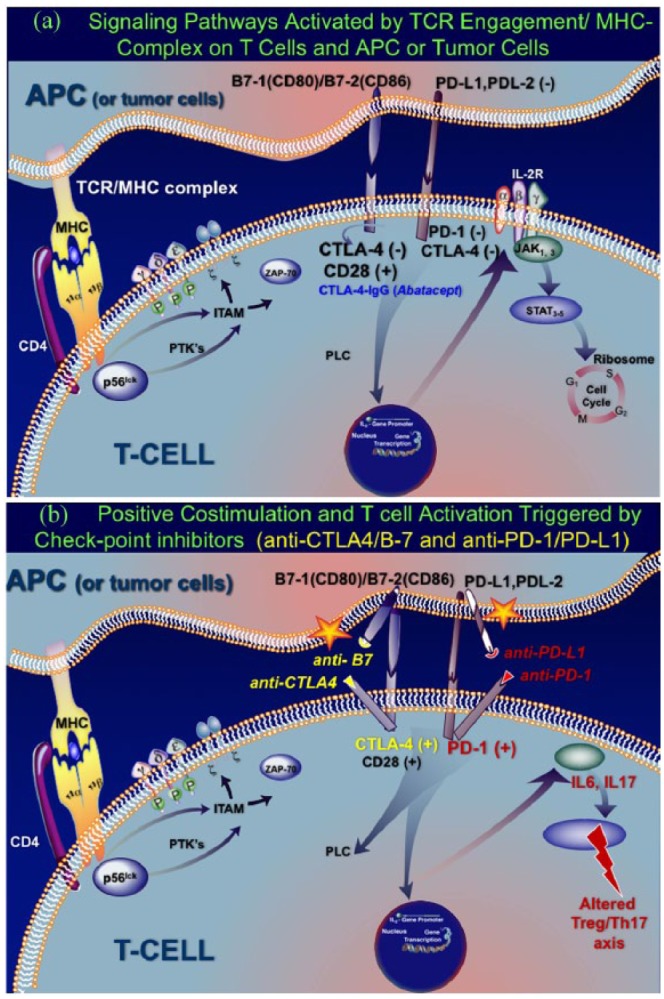
Patients with advanced malignancies treated with immune checkpoint inhibitors are at increased risk for developing immune-related neurological complications. It is a phenomenon of immunological twist when immunotherapy against co-stimulatory molecules activates previously normal T cells to kill tumor cells but, in so doing, the T cells become unrestrained, triggering other autoimmune diseases for which conventional immunotherapy is needed. The most common autoimmune neurological diseases, usually occurring within 2-12 weeks after immune checkpoint inhibitor initiation, include: inflammatory myopathies, myasthenia gravis, acute and chronic demyelinating polyradiculoneuropathies, vasculitic neuropathies, isolated cranial neuropathies, aseptic meningitis, autoimmune encephalitis, multiple sclerosis and hypophysitis. The neurological events can evolve rapidly, necessitating the need for vigilance at all stages of treatment, even after completion, because early immunotherapeutic interventions are effective. The review addresses these complications and the applied therapies, discusses immune pathomechanisms including triggering preexisting autoimmunity, highlights the distinction between paraneoplastic and autoimmune etiologies, and identifies uncertainties regarding risk factors, use of immune checkpoint inhibitors in patients with known immune diseases or restarting therapy after a neurological event. Although the autoimmune neurological complications are not very common, their incidence will likely increase as the use of immune checkpoint inhibitors in metastatic cancer is growing rapidly.
Keywords: autoimmune neurological disorders; immune checkpoint inhibitors; immune-related neurological complications; immunotherapy; neuro-immunology; neurological side effects.
Conflict of interest statement
Conflict of interest statement: The author declares that there is no conflict of interest.
Figures
References
-
- Postow MA, Sidlow R, Hellmann MD. Immune-related adverse events associated with immune checkpoint blockade. N Engl J Med 2018; 378: 158–168. - PubMed
-
- Fellner A, Makranz C, Lotem M, et al. Neurologic complications of immune checkpoint inhibitors. J Neuro-Oncology 2018; 137: 601–609. - PubMed
-
- Astaras C, Michell R, Moura B, et al. Neurological adverse events associated with immune checkpoint inhibitors: diagnosis and management. Curr Neurol Neurosci Rep 2018; 18: 3. - PubMed
-
- Hottinger AF. Neurologic complications of immune checkpoint inhibitors. Curr Opin Neurol 2016; 29: 806–812. - PubMed
-
- Wick W, Hertenstein A, Platten M. Neurological sequelae of cancer immunotherapies and targeted therapies. Lancet Oncol 2016; 17: e529–e541. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
