Instrument flight to the inner ear
- PMID: 30246168
- PMCID: PMC6150423
- DOI: 10.1126/scirobotics.aal4916
Instrument flight to the inner ear
Abstract
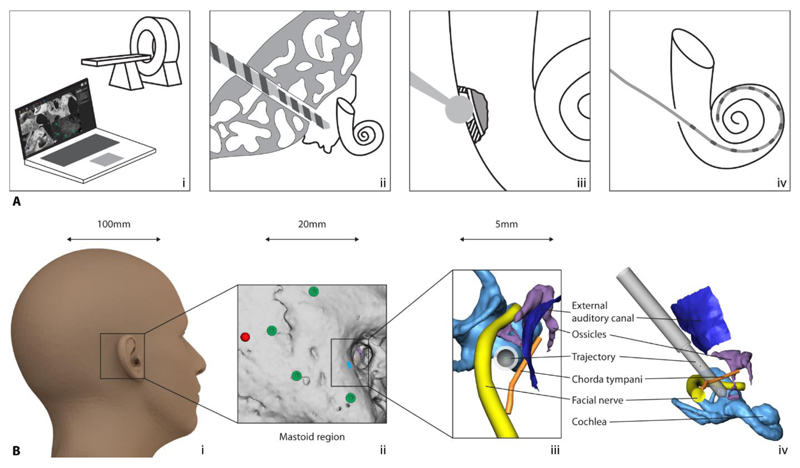
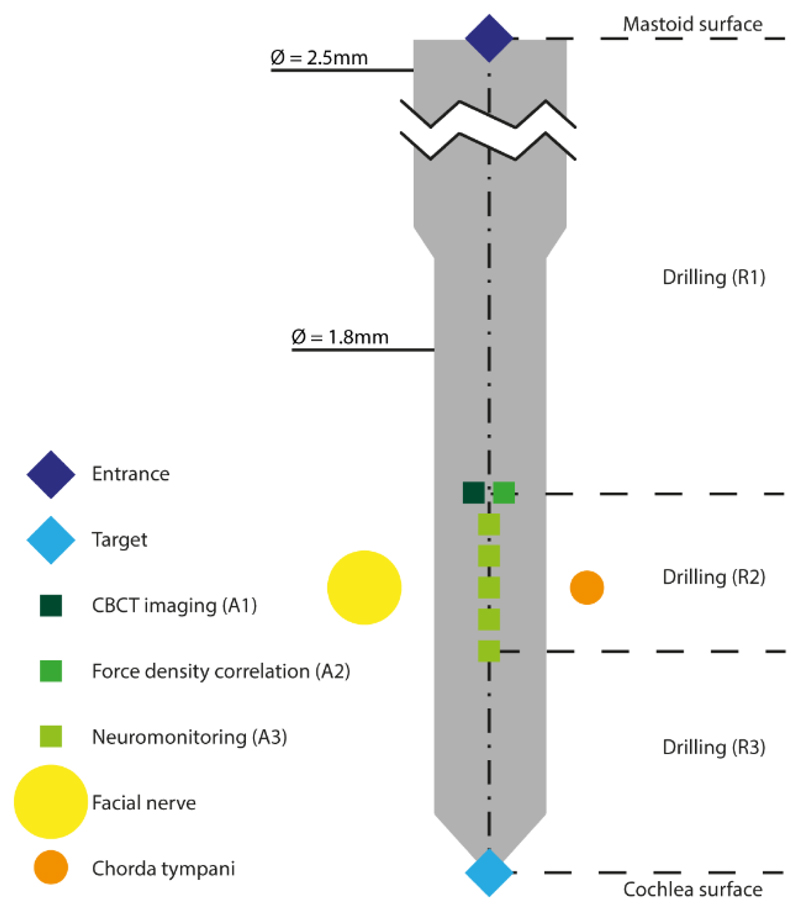
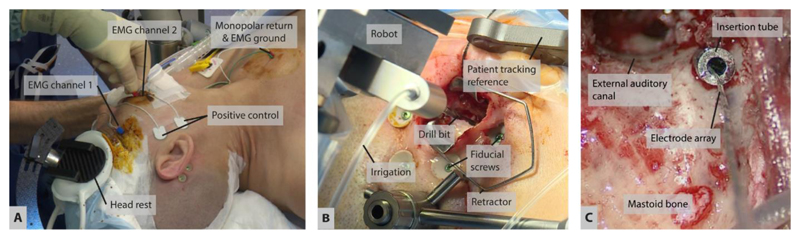
Surgical robot systems can work beyond the limits of human perception, dexterity and scale making them inherently suitable for use in microsurgical procedures. However, despite extensive research, image-guided robotics applications for microsurgery have seen limited introduction into clinical care to date. Among others, challenges are geometric scale and haptic resolution at which the surgeon cannot sufficiently control a device outside the range of human faculties. Mechanisms are required to ascertain redundant control on process variables that ensure safety of the device, much like instrument-flight in avionics. Cochlear implantation surgery is a microsurgical procedure, in which specific tasks are at sub-millimetric scale and exceed reliable visuo-tactile feedback. Cochlear implantation is subject to intra- and inter-operative variations, leading to potentially inconsistent clinical and audiological outcomes for patients. The concept of robotic cochlear implantation aims to increase consistency of surgical outcomes such as preservation of residual hearing and reduce invasiveness of the procedure. We report successful image-guided, robotic CI in human. The robotic treatment model encompasses: computer-assisted surgery planning, precision stereotactic image-guidance, in-situ assessment of tissue properties and multipolar neuromonitoring (NM), all based on in vitro, in vivo and pilot data. The model is expandable to integrate additional robotic functionalities such as cochlear access and electrode insertion. Our results demonstrate the feasibility and possibilities of using robotic technology for microsurgery on the lateral skull base. It has the potential for benefit in other microsurgical domains for which there is no task-oriented, robotic technology available at present.
Conflict of interest statement
Competing interests: B.B., T.W., S.W. are inventors on the related patent: EP2666248; A.F., S.W. are inventors on the related patent EP16153033.S.W. is co-founder, shareholder and advisor to the board and M.M. is chief technology officer and shareholder of CAScination AG (Bern Switzerland), a company that is developing robotic cochlear implantation technology. MC is a member of the scientific advisory board and M.K. received travel funding from MED-EL GmbH (Innsbruck, Austria), a cochlear implant company.
Figures
References
-
- Agin GJ. Technical Note 179. SRI International; 1979. Feb, Real Time Control of a Robot with a Mobile Camera.
-
- Airframe and Powerplant Mechanics Airframe Handbook (Publication AC65-15A) Washington, DC: US Department of Transportation Federal Aviation Administration Standards Division; 1976. p. 4. ISBN 0-16-036209-1.
-
- Ansó J, Dür C, Gavaghan K, Rohrbach H, Gerber N, Williamson T, et al. A Neuromonitoring Approach to Facial Nerve Preservation During Image-guided Robotic Cochlear Implantation. Otol Neurotol. 2016;37:89–98. - PubMed
-
- Bielamowicz S, Coker N, Jenkins H, Igarashi M. Surgical dimensions of the facial recess in adults and children. Arch Otolaryngol Head Neck Surg. 1988 May;114(5):534–7. - PubMed
-
- Bell B, Williamson T, Gerber N, Gavaghan K, Wimmer W, Caversaccio M, Weber S. In Vitro Accuracy Evaluation of Image-Guided Robot System for Direct Cochlear Access. Otol Neurotol. 2013;34:1284–90. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources