

Attributable Cost of Dementia: Demonstrating Pitfalls of Ignoring Multiple Health Care System Utilization
- PMID: 30246404
- PMCID: PMC6235812
- DOI: 10.1111/1475-6773.13048
Attributable Cost of Dementia: Demonstrating Pitfalls of Ignoring Multiple Health Care System Utilization
Abstract
Objectives: To determine dementia prevalence and costs attributable to dementia using Veterans Health Administration (VHA) data with and without Medicare data.
Data sources: VHA inpatient, outpatient, purchased care and other data and Medicare enrollment, claims, and assessments in fiscal year (FY) 2013.
Study design: Analyses were conducted with VHA data alone and with combined VHA and Medicare data. Dementia was identified from a VHA sanctioned list of ICD-9 diagnoses. Attributable cost of dementia was estimated using recycled predictions.
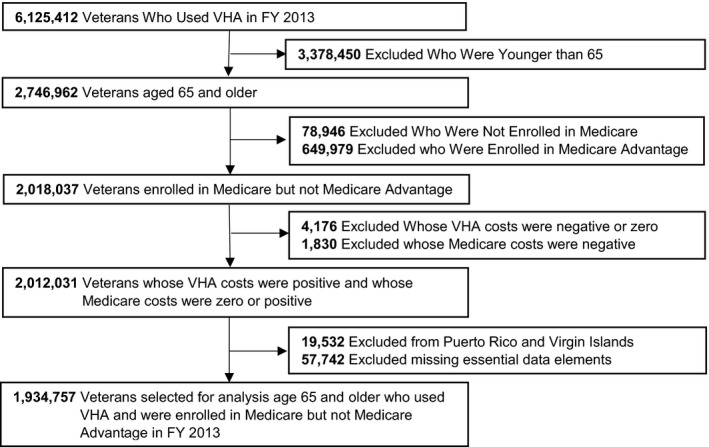
Data collection: Veterans age 65 and older who used VHA and were enrolled in Traditional Medicare in FY 2013 (1.9 million).
Principal findings: VHA records indicated the prevalence of dementia in FY 2013 was 4.8 percent while combined VHA and Medicare data indicated the prevalence was 7.4 percent. Attributable cost of dementia to VHA was, on average, $10,950 per veteran per year (pvpy) using VHA alone and $6,662 pvpy using combined VHA and Medicare data. Combined VHA and Medicare attributable cost of dementia was $11,285 pvpy. Utilization attributed to dementia using VHA data alone was lower for long-term institutionalization and higher for supportive care services than indicated in combined VHA and Medicare data.
Conclusions: Better planning for clinical and cost-efficient care requires VHA and Medicare to share data for veterans with dementia and likely more generally.
Keywords: Health care costs; VA Health Care System; medicaid; medicare.
© Health Research and Educational Trust.
Figures
Similar articles
-
Continuity of care and health care cost among community-dwelling older adult veterans living with dementia.Health Serv Res. 2021 Jun;56(3):378-388. doi: 10.1111/1475-6773.13541. Epub 2020 Aug 19. Health Serv Res. 2021. PMID: 32812658 Free PMC article.
-
Using the Medicare Current Beneficiary Survey to conduct research on Medicare-eligible veterans.J Rehabil Res Dev. 2010;47(8):797-813. doi: 10.1682/jrrd.2009.10.0174. J Rehabil Res Dev. 2010. PMID: 21110253
-
Medical foster home is less costly than traditional nursing home care.Health Serv Res. 2019 Dec;54(6):1346-1356. doi: 10.1111/1475-6773.13195. Epub 2019 Jul 22. Health Serv Res. 2019. PMID: 31328798 Free PMC article.
-
Cost of dementia in Medicare managed care: a systematic literature review.Am J Manag Care. 2019 Aug 1;25(8):e247-e253. Am J Manag Care. 2019. PMID: 31419102 Free PMC article.
-
Skilled home healthcare utilization and outcomes for older adults with dementia: A scoping review.J Am Geriatr Soc. 2025 Feb;73(2):612-625. doi: 10.1111/jgs.19203. Epub 2024 Oct 2. J Am Geriatr Soc. 2025. PMID: 39355968
Cited by
-
Demographic, Health, and Exposure Risks Associated With Cognitive Loss, Alzheimer's Disease and Other Dementias in US Military Veterans.Front Psychiatry. 2021 Feb 25;12:610334. doi: 10.3389/fpsyt.2021.610334. eCollection 2021. Front Psychiatry. 2021. PMID: 33716816 Free PMC article. Review.
-
HSR Commentary: Linking VA and Non-VA Data to Address Important US Veteran Health Services Research Issues.Health Serv Res. 2018 Dec;53 Suppl 3(Suppl Suppl 3):5133-5139. doi: 10.1111/1475-6773.13081. Health Serv Res. 2018. PMID: 30430570 Free PMC article.
-
Increased Risk of Dementia Among Veterans With Bipolar Disorder or Schizophrenia Receiving Care in the VA Health System.Psychiatr Serv. 2020 Oct 1;71(10):998-1004. doi: 10.1176/appi.ps.201900325. Epub 2020 Jun 10. Psychiatr Serv. 2020. PMID: 32517643 Free PMC article.
-
Comparison of Japanese Centenarians' and Noncentenarians' Medical Expenditures in the Last Year of Life.JAMA Netw Open. 2021 Nov 1;4(11):e2131884. doi: 10.1001/jamanetworkopen.2021.31884. JAMA Netw Open. 2021. PMID: 34739063 Free PMC article.
-
Regional Differences in Dementia Incidence Among US Veterans.JAMA Neurol. 2025 Jun 9;82(8):817-24. doi: 10.1001/jamaneurol.2025.1536. Online ahead of print. JAMA Neurol. 2025. PMID: 40489088
References
-
- Akushevich, I. , Yashkin A., Kravchenko J., Ukraintseva S., Stallard E., and Yashin A. I.. 2018. “Time Trends in the Prevalence of Neurocognitive Disorders and Cognitive Impairment in the United States: The Effects of Disease Severity and Improved Ascertainment.” Journal of Alzheimer's Disease (Preprint): 1–12, 53 (6): 5330–50. - PMC - PubMed
-
- Alzheimer's Association . 2017. “2017 Alzheimer's Disease Facts and Figures.” Alzheimer's & Dementia 13 (4): 325–73.
-
- Bynum, J. P. , Rabins P. V., Weller W., Niefeld M., Anderson G. F., and Wu A. W.. 2004. “The Relationship between a Dementia Diagnosis, Chronic Illness, Medicare Expenditures, and Hospital Use.” Journal of the American Geriatrics Society 52 (2): 187–94. - PubMed
-
- Byrne, M. M. , Kuebeler M., Pietz K., and Petersen L. A.. 2006. “Effect of Using Information from Only One System for Dually Eligible Health Care Users.” Medical Care 44 (8): 768–73. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
