

Role of the status of the mesorectal fascia in the selection of patients with rectal cancer for preoperative radiation therapy: a retrospective cohort study
- PMID: 30247008
- PMCID: PMC6153109
- DOI: 10.1503/cjs.009417
Role of the status of the mesorectal fascia in the selection of patients with rectal cancer for preoperative radiation therapy: a retrospective cohort study
Abstract
Background: Patients with rectal cancer in whom the mesorectal fascia is threatened by tumour are more likely than all patients with stage II/III disease to benefit from preoperative radiotherapy (RT). The objective of this study was to assess whether the status of the mesorectal fascia versus a stage II/III designation can best inform the use of preoperative RT in patients undergoing major rectal cancer resection.
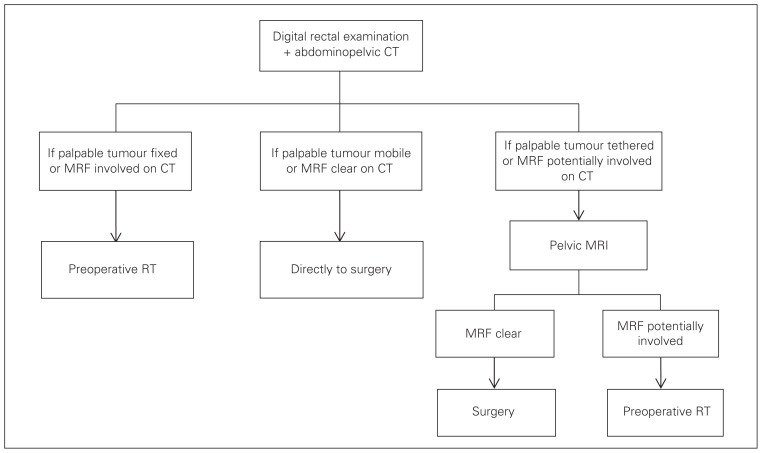
Methods: We reviewed the charts of consecutive patients with primary rectal cancer treated by a single surgeon at McMaster University, Hamilton, Ontario, between March 2006 and December 2012. The status of the mesorectal fascia was assessed by digital rectal examination, pelvic computed tomography and, when needed, pelvic magnetic resonance imaging (MRI). Patients whose mesorectal fascia was threatened or involved by tumour received preoperative RT. The study outcomes were rates of positive circumferential radial margin (CRM) and local tumour recurrence.
Results: A total of 153 patients were included, of whom 76 (49.7%) received preoperative RT because of concerns of a compromised mesorectal fascia. The median length of follow-up was 4.5 years. The number of CRM-positive cases in the RT and no-RT groups was 16 (22%) and 1 (1%), respectively (p < 0.01), and the number of cases of local tumour recurrence was 5 (7%) and 2 (3%), respectively (p = 0.2). Rates were similar when only patients with stage II/III tumours were included. Overall, 26 patients (17.0%) received MRI.
Conclusion: The status of the mesorectal fascia, not tumour stage, may best identify patients for preoperative RT.
Contexte: Plus que tous les patients présentant une maladie de stade II/III, les patients atteints d’un cancer du rectum dont le fascia mésorectal est menacé par la tumeur sont de bons candidats à la radiothérapie (RT) préopératoire. L’objectif de cette étude était d’évaluer ce qui, entre l’état du fascia mésorectal et une désignation de stade II/III, permet le mieux de confirmer le bien-fondé d’une RT préopératoire chez les patients qui doivent subir une résection majeure pour cancer du rectum.
Méthodes: Nous avons passé en revue les dossiers de patients consécutifs atteints d’un cancer rectal primaire traités par un seul chirurgien à l’Université McMaster, à Hamilton, en Ontario, entre mars 2006 et décembre 2012. L’état du fascia mésorectal a été évalué par toucher rectal, tomodensitométrie pelvienne et, au besoin, imagerie par résonnance magnétique (IRM) pelvienne. Les patients dont le fascia mésorectal était menacé ou affecté par la tumeur ont reçu une RT préopératoire. Les paramètres de l’étude étaient : taux de positivité de la marge radiale circonférentielle (MRC) et récurrence de la tumeur locale.
Résultats: En tout, 153 patients ont été inclus, dont 76 (49,7 %) ont reçu une RT préopératoire en raison d’une atteinte du fascia mésorectal. La durée moyenne du suivi a été de 4,5 ans. Dans les groupes soumis et non soumis à la RT, les nombres de cas MRC-positifs ont été respectivement de 16 (22 %) et de 1 (1 %), (p < 0,01), et les nombres de cas de récurrence de la tumeur locale ont été respectivement de 5 (7 %) et de 2 (3 %) (p = 0,2). Les taux étaient similaires lorsque seuls les patients présentant des tumeurs de stade II/III étaient inclus. Globalement, 26 patients (17,0 %) ont subi l’IRM.
Conclusion: C’est l’état du fascia mésorectal et non le stade de la tumeur qui peut le mieux permettre d’identifier les candidats à une RT préopératoire.
Conflict of interest statement
None declared.
Figures
Similar articles
-
Circumferential resection margin positivity after preoperative chemoradiotherapy based on magnetic resonance imaging for locally advanced rectal cancer: implication of boost radiotherapy to the involved mesorectal fascia.Jpn J Clin Oncol. 2016 Apr;46(4):316-22. doi: 10.1093/jjco/hyv208. Epub 2016 Jan 21. Jpn J Clin Oncol. 2016. PMID: 26802164 Free PMC article.
-
Can CT replace MRI in preoperative assessment of the circumferential resection margin in rectal cancer?Dis Colon Rectum. 2010 Mar;53(3):308-14. doi: 10.1007/DCR.0b013e3181c5321e. Dis Colon Rectum. 2010. PMID: 20173478
-
Why did we encounter a pCRM-positive specimen whose preoperative MRI indicates negative mesorectal fascia involvement in middle to low rectal cancer?Tech Coloproctol. 2025 Mar 17;29(1):81. doi: 10.1007/s10151-025-03117-3. Tech Coloproctol. 2025. PMID: 40095215 Free PMC article.
-
[The role of magnetic resonance imaging to select patients for preoperative treatment in rectal cancer].Strahlenther Onkol. 2009 Aug;185(8):488-92. doi: 10.1007/s00066-009-2043-3. Epub 2009 Aug 4. Strahlenther Onkol. 2009. PMID: 19652930 Review. German.
-
The clinical significance of the circumferential resection margin following preoperative pelvic chemo-radiotherapy in rectal cancer: why we need a common language.Colorectal Dis. 2006 Nov;8(9):800-7. doi: 10.1111/j.1463-1318.2006.01139.x. Colorectal Dis. 2006. PMID: 17032329 Review.
Cited by
-
Synthetic magnetic resonance imaging predicts the prognostic evaluation of rectal cancer.Quant Imaging Med Surg. 2023 Mar 1;13(3):2026-2028. doi: 10.21037/qims-22-624. Epub 2022 Oct 19. Quant Imaging Med Surg. 2023. PMID: 36915299 Free PMC article. No abstract available.
-
Identification of patients with locally advanced rectal cancer eligible for neoadjuvant chemotherapy alone: Results of a retrospective study.Cancer Med. 2023 Jun;12(12):13309-13318. doi: 10.1002/cam4.6029. Epub 2023 May 6. Cancer Med. 2023. PMID: 37148548 Free PMC article.
References
-
- Martling AL, Holm T, Rutqvist LE, et al. Effect of a surgical training programme on outcome of rectal cancer in the country of Stokholm. Stockholm Colorectal Cancer Study Group, Basingstoke Bowel Cancer Research Project. Lancet. 2000;356:93–6. - PubMed
-
- Kapiteijn E, Marijnen CA, Colenbrander AC, et al. Local recurrence in patients with rectal cancer diagnosed between 1988 and 1992: a population-based study in the west Netherlands. Eur J Surg Oncol. 1998;24:528–35. - PubMed
-
- Heald RJ, Moran BJ, Ryall RDH, et al. Rectal cancer: the Basingstoke experience of total mesorectal excision, 1978–1997. Arch Surg. 1998;133:894–9. - PubMed
-
- Peeters KCMJ, Marijnen CAM, Nagtegaal ID, et al. The TME trial after a median follow-up of 6 years: increased local control but no survival benefit in irradiated patients with resectable rectal carcinoma. Ann Surg. 2007;246:693–701. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical