

Inflammation, Active Fibroplasia, and End-stage Fibrosis in 172 Biliary Atresia Remnants Correlate Poorly With Age at Kasai Portoenterostomy, Visceral Heterotaxy, and Outcome
- PMID: 30247160
- PMCID: PMC6637020
- DOI: 10.1097/PAS.0000000000001146
Inflammation, Active Fibroplasia, and End-stage Fibrosis in 172 Biliary Atresia Remnants Correlate Poorly With Age at Kasai Portoenterostomy, Visceral Heterotaxy, and Outcome
Abstract
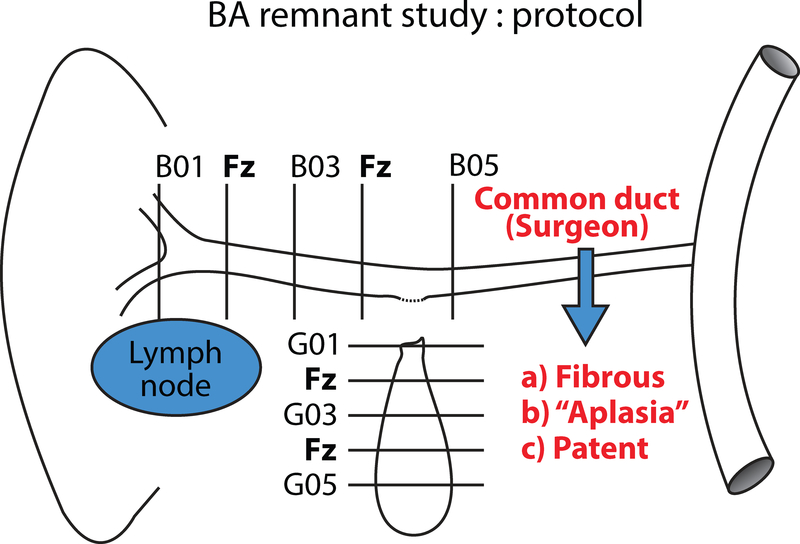
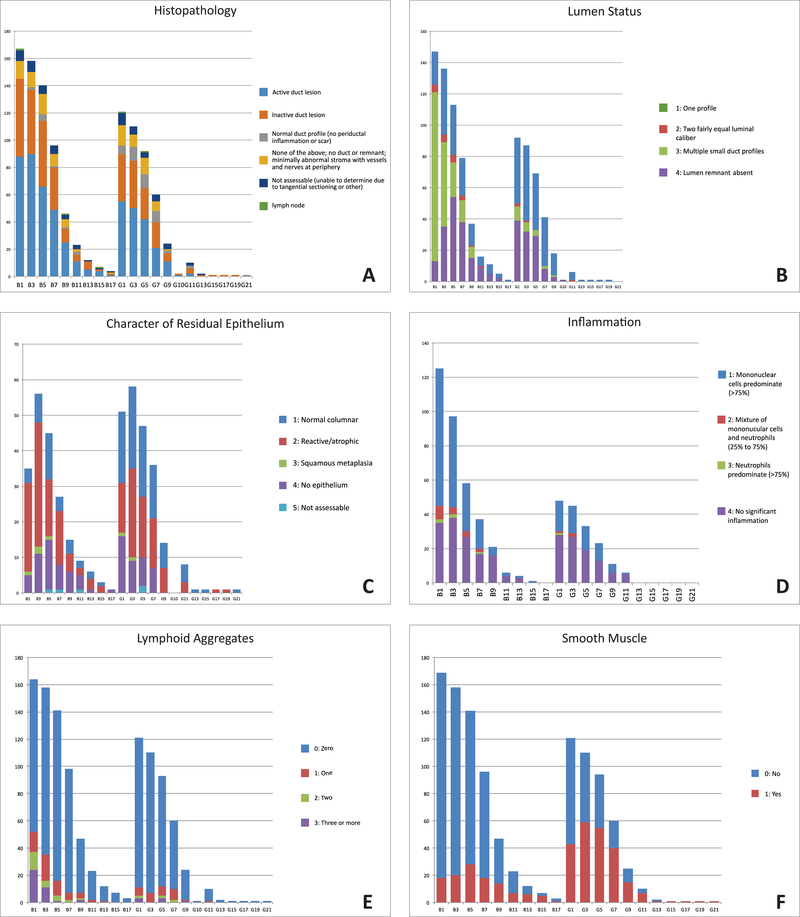
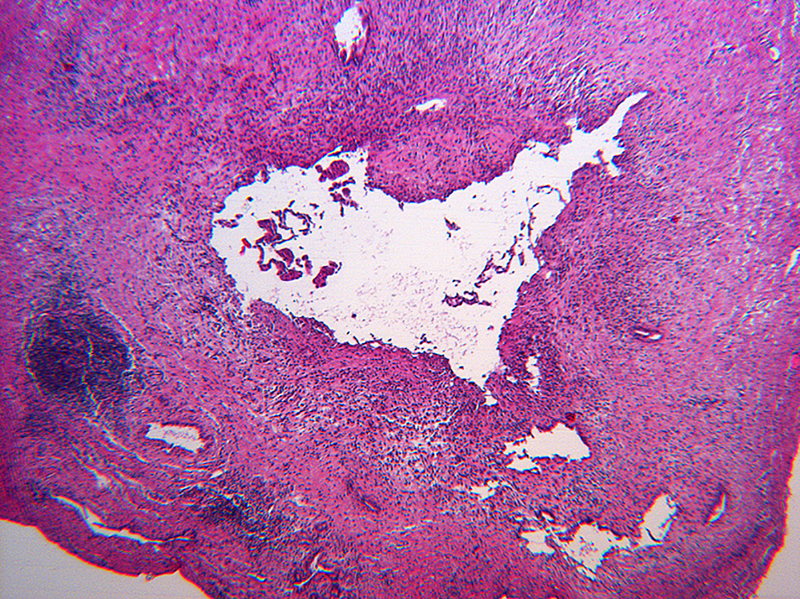
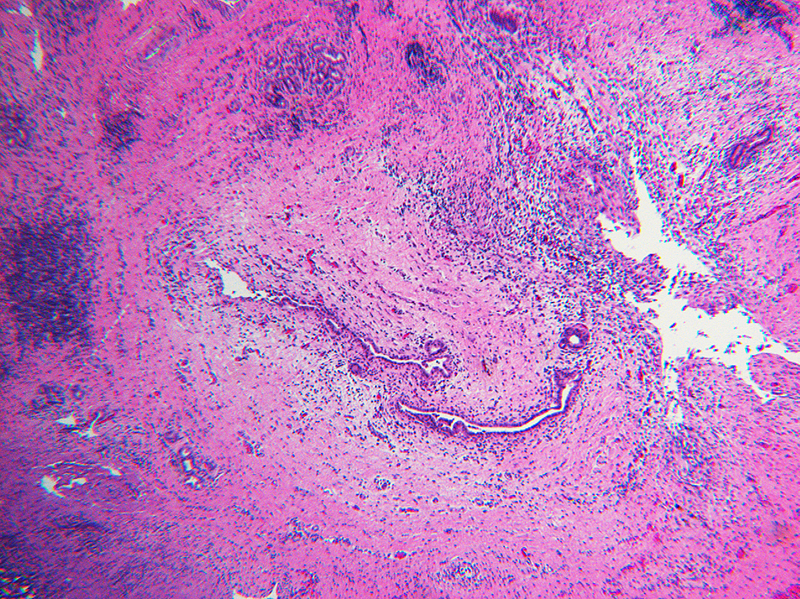
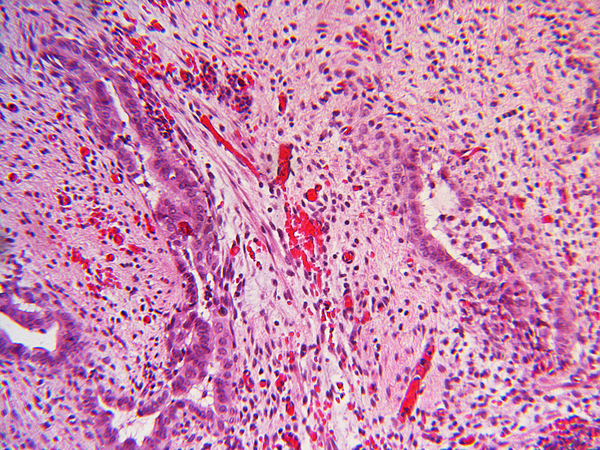
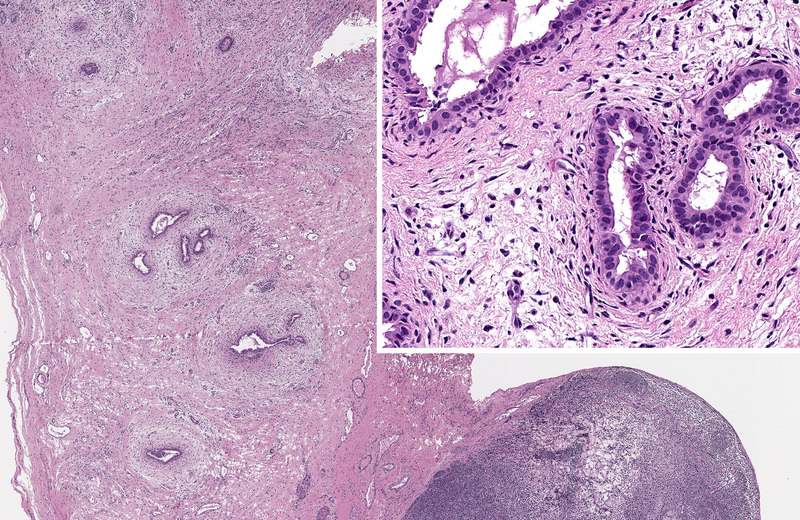
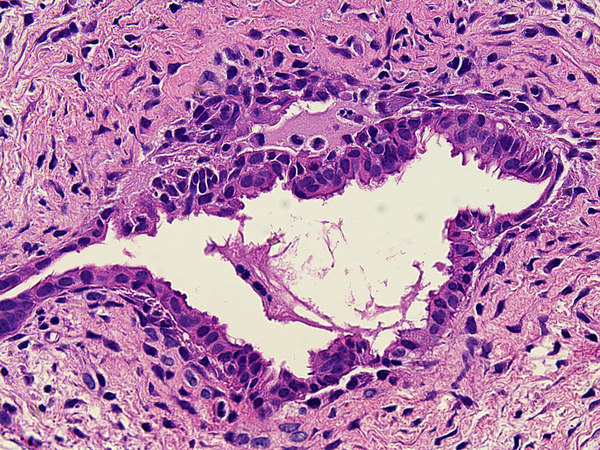
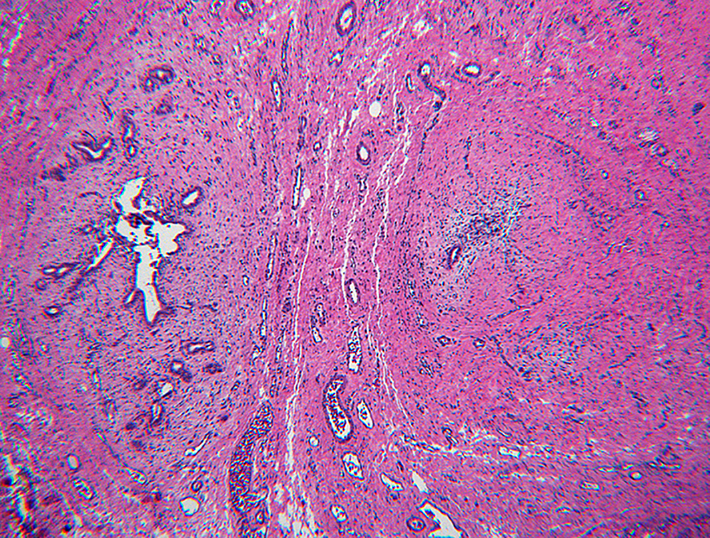
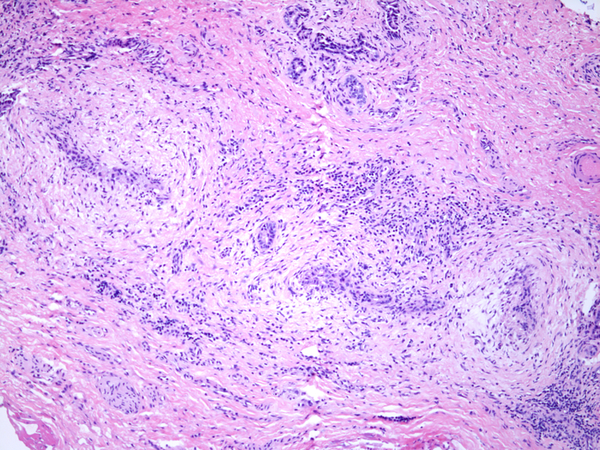
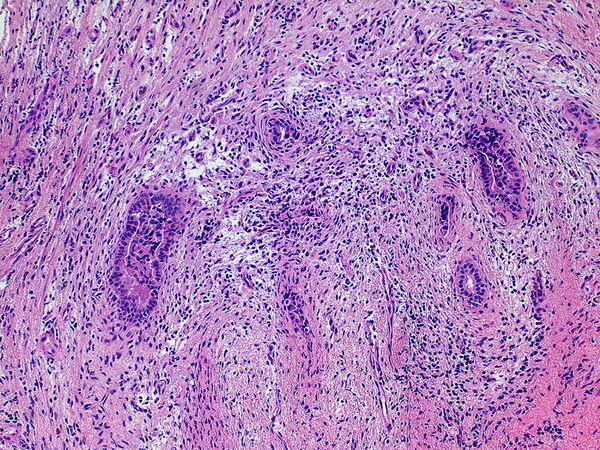
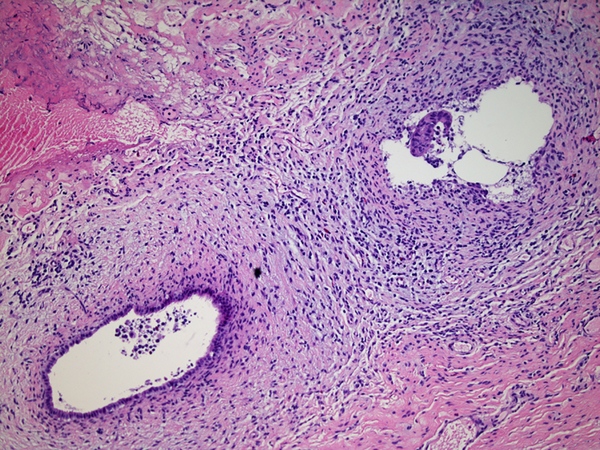
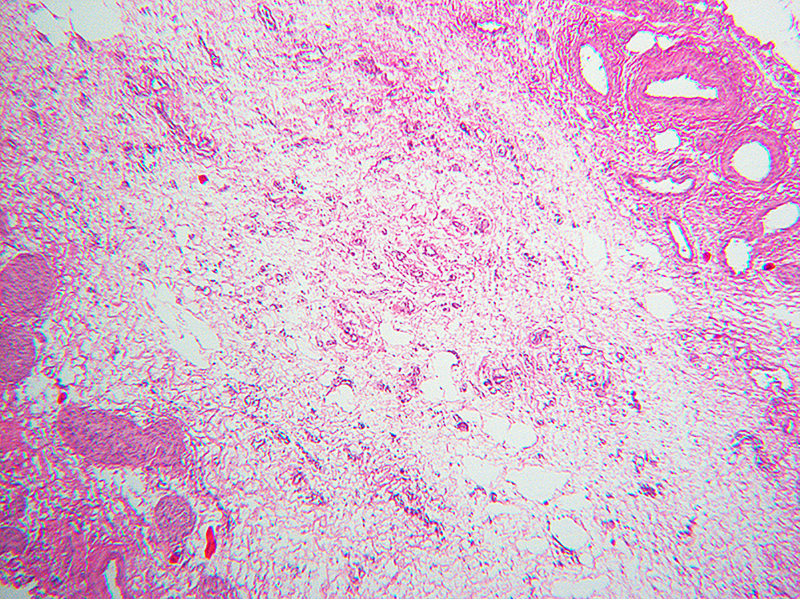
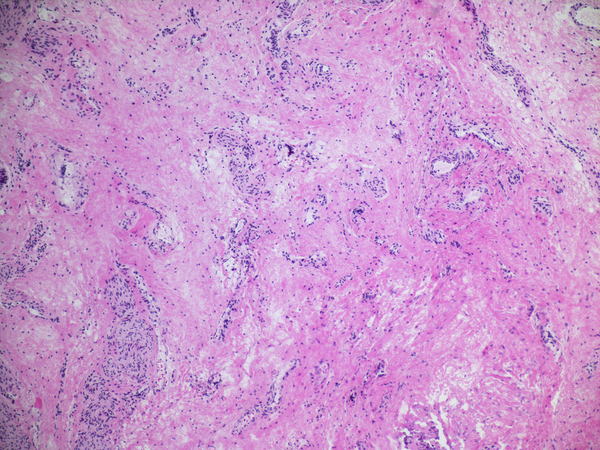
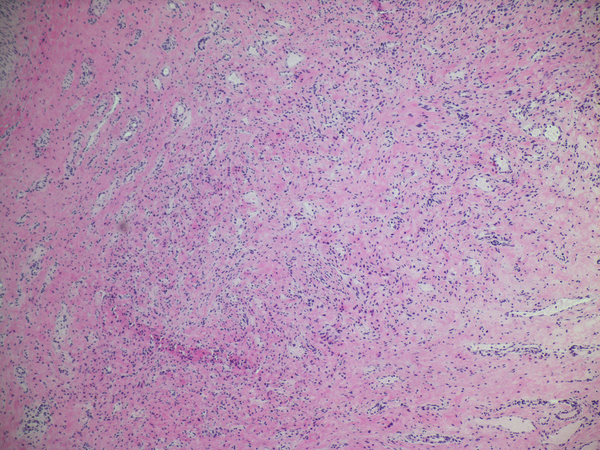
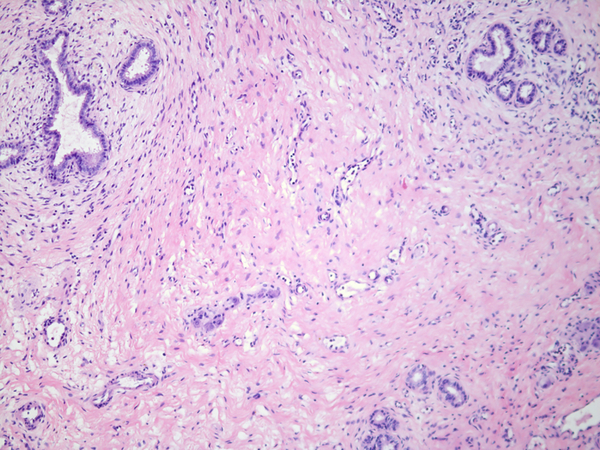
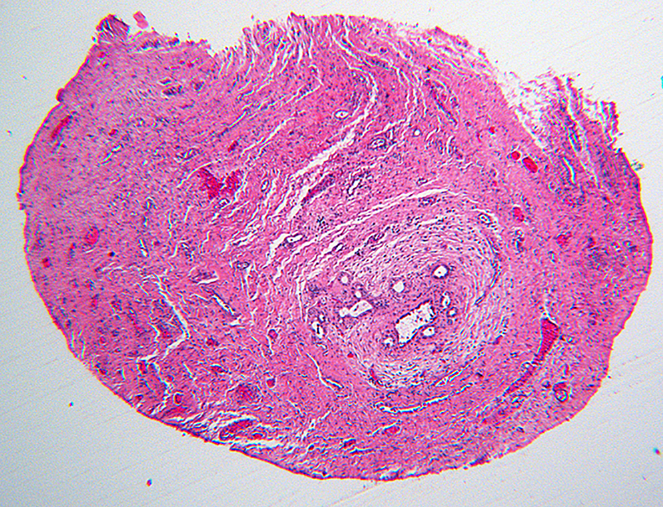
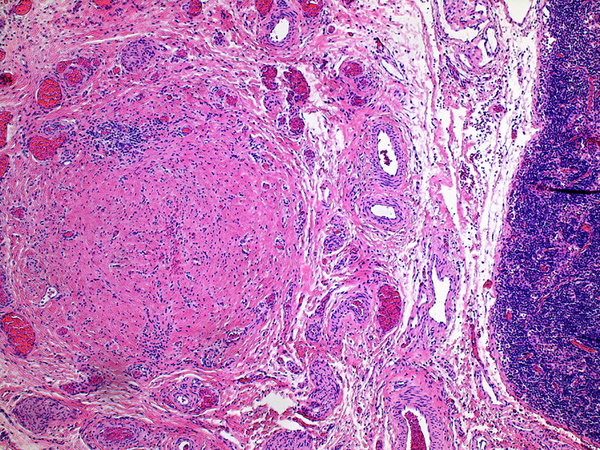
Published histologic studies of the hilar plate or entire biliary remnant at the time of Kasai portoenterostomy (KHPE) have not provided deep insight into the pathogenesis of biliary atresia, relation to age at surgery, prognosis or the basis for successful drainage. We report detailed histologic findings in 172 centrally reviewed biliary remnants with an average of 6 sections per subject. Active lesions were classified as either necroinflammatory (rare/clustered in a few subjects) or active concentric fibroplasia with or without inflammation (common). Inactive lesions showed bland replacement by collagen and fibrous cords with little or no inflammation. Heterogeneity was common within a given remnant; however, relatively homogenous histologic patterns, defined as 3 or more inactive or active levels in the hepatic ducts levels, characterized most remnants. Homogeneity did not correlate with age at KHPE, presence/absence of congenital anomalies at laparotomy indicative of heterotaxy and outcome. Remnants from youngest subjects were more likely than older subjects to be homogenously inactive suggesting significantly earlier onset in the youngest subset. Conversely remnants from the oldest subjects were often homogenously active suggesting later onset or slower progression. More data are needed in remnants from subjects <30 days old at KHPE and in those with visceral anomalies. Prevalence of partially preserved epithelium in active fibroplastic biliary atresia lesions at all ages suggests that epithelial regression or injury may not be a primary event or that reepithelialization is already underway at the time of KHPE. We hypothesize that outcome after KHPE results from competition between active fibroplasia and reepithelialization of retained, collapsed but not obliterated lumens. The driver of active fibroplasia is unknown.
Figures

Similar articles
-
Hepatic Hilar Lymph Node Reactivity at Kasai Portoenterostomy for Biliary Atresia: Correlations With Age, Outcome, and Histology of Proximal Biliary Remnant.Pediatr Dev Pathol. 2018 Jan-Feb;21(1):29-40. doi: 10.1177/1093526617707851. Epub 2017 May 5. Pediatr Dev Pathol. 2018. PMID: 28474973 Free PMC article.
-
Biliary atresia--a fifteen-year review of clinical and pathologic factors associated with liver transplantation.J Pediatr Surg. 2004 Jun;39(6):800-3. doi: 10.1016/j.jpedsurg.2004.02.020. J Pediatr Surg. 2004. PMID: 15185199 Review.
-
Effect of repeat Kasai hepatic portoenterostomy on pediatric live-donor liver graft for biliary atresia.Exp Clin Transplant. 2013 Jun;11(3):259-63. doi: 10.6002/ect.2012.0188. Epub 2013 Mar 26. Exp Clin Transplant. 2013. PMID: 23530849
-
Past and future of biliary atresia.J Pediatr Surg. 2000 May;35(5):717-20. doi: 10.1053/jpsu.2000.6034. J Pediatr Surg. 2000. PMID: 10813333
-
Biliary atresia--surgical management and treatment options as they relate to outcome.Liver Transpl Surg. 1998 Sep;4(5 Suppl 1):S24-33. Liver Transpl Surg. 1998. PMID: 9742491 Review.
Cited by
-
Recent developments in etiology and disease modeling of biliary atresia: a narrative review.Dig Med Res. 2020 Dec;3:59. doi: 10.21037/dmr-20-97. Dig Med Res. 2020. PMID: 33615212 Free PMC article.
-
Cellular crosstalk mediated by TGF-β drives epithelial-mesenchymal transition in patient-derived multi-compartment biliary organoids.Nat Commun. 2025 Jul 17;16(1):6575. doi: 10.1038/s41467-025-61442-5. Nat Commun. 2025. PMID: 40675983 Free PMC article.
-
In Utero Extrahepatic Bile Duct Damage and Repair: Implications for Biliary Atresia.Pediatr Dev Pathol. 2024 Jul-Aug;27(4):291-310. doi: 10.1177/10935266241247479. Epub 2024 May 19. Pediatr Dev Pathol. 2024. PMID: 38762769 Free PMC article. Review.
-
Biliary Atresia Animal Models: Is the Needle in a Haystack?Int J Mol Sci. 2022 Jul 16;23(14):7838. doi: 10.3390/ijms23147838. Int J Mol Sci. 2022. PMID: 35887185 Free PMC article. Review.
References
-
- Gautier M, Jehan P, Odievre M. Histologic Study of biliary fibrous remnants in 48 cases of extrahepatic biliary atresia: correlation with postoperative bile flow restoration. J Pediatr. 1976;89:704–9. - PubMed
-
- Gautier M Atresia of the extrahepatic bile ducts. Etiologic hypothesis founded on a histological study of 130 fibrous remnants. Arch Fr Pediatr. 1979;36(9 suppl):III–XII. - PubMed
Publication types
MeSH terms
Grants and funding
- U01 DK062481/DK/NIDDK NIH HHS/United States
- U01 DK062470/DK/NIDDK NIH HHS/United States
- U01 DK062436/DK/NIDDK NIH HHS/United States
- U01 DK062452/DK/NIDDK NIH HHS/United States
- U01 DK062466/DK/NIDDK NIH HHS/United States
- U01 DK084575/DK/NIDDK NIH HHS/United States
- U01 DK084536/DK/NIDDK NIH HHS/United States
- U01 DK062456/DK/NIDDK NIH HHS/United States
- U01 DK062445/DK/NIDDK NIH HHS/United States
- U01 DK103149/DK/NIDDK NIH HHS/United States
- U24 DK062456/DK/NIDDK NIH HHS/United States
- U01 DK084538/DK/NIDDK NIH HHS/United States
- U01 DK062453/DK/NIDDK NIH HHS/United States
- U01 DK062503/DK/NIDDK NIH HHS/United States
- U01 DK062500/DK/NIDDK NIH HHS/United States
- U01 DK062497/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
