

Neutralizing Peripheral Refraction Eliminates Refractive Scotomata in Tilted Disc Syndrome
- PMID: 30247238
- PMCID: PMC6166693
- DOI: 10.1097/OPX.0000000000001286
Neutralizing Peripheral Refraction Eliminates Refractive Scotomata in Tilted Disc Syndrome
Abstract
Significance: We demonstrate that the visual field defects in patients with tilted disc syndrome can be reduced or eliminated by neutralizing the peripheral scotoma in the area of posterior retinal bowing, which may allow differentiation between a congenital anomaly and acquired pathology.
Purpose: Tilted disc syndrome is a congenital and unchanging condition that may present with visual field defects mimicking loss seen in neurological diseases, such as transsynaptic retrograde degeneration. Our purpose was to systematically investigate the ability of a neutralized peripheral refraction to eliminate refractive visual field defects seen in tilted disc syndrome. This was compared with the same technique performed on patients with neurological deficits.
Methods: The Humphrey Field Analyzer was used to measure sensitivities across the 30-2 test grid in 14 patients with tilted disc syndrome using four refractive corrections: habitual near correction and with an additional -1.00, -2.00 or -3.00 D negative lens added as correction lenses. Peripheral refractive errors along the horizontal meridian were determined using peripheral retinoscopy and thus allowed calculation of residual peripheral refraction with different levels of refractive correction. Visual field defects were assessed qualitatively and quantitatively using sensitivities and probability scores in both patient groups.
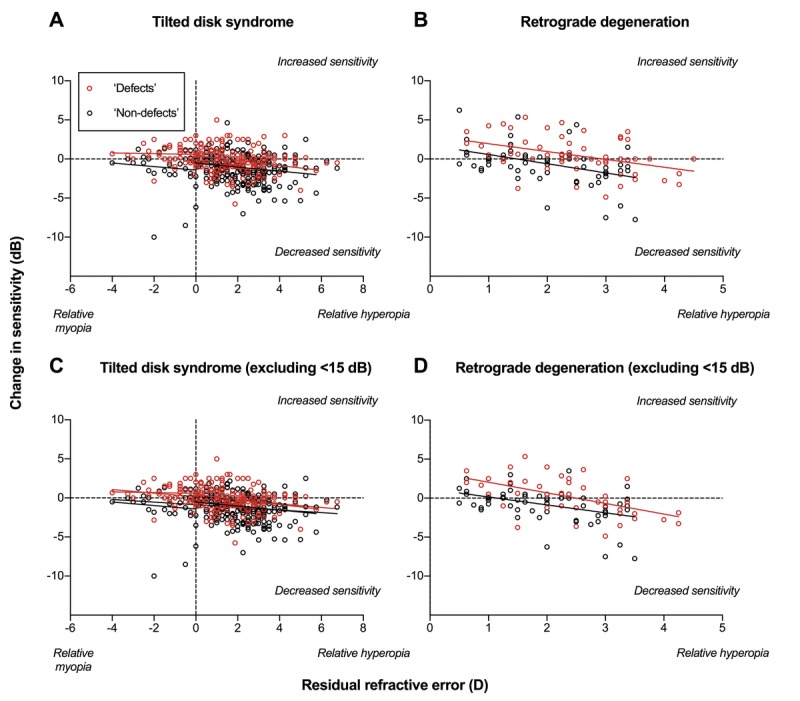
Results: A smaller residual refractive error after the application of negative addition lenses correlated with improvement in visual field defects in terms of sensitivity and probability scores in patients with tilted disc syndrome. Patients with established neurological deficits (retrograde degeneration) showed improvement in sensitivities but not in probability scores.
Conclusions: Neutralizing the refractive error at the region of posterior retinal bowing due to tilted disc syndrome reduces the apparent visual field defect. This may be a useful and rapid test to help differentiate between tilted disc syndrome and other pathological causes of visual field defects such as neurological deficits.
Conflict of interest statement
Figures






References
-
- Witmer MT, Margo CE, Drucker M. Tilted Optic Disks. Surv Ophthalmol 2010;55:403–28. - PubMed
-
- How AC, Tan GS, Chan YH, et al. Population Prevalence of Tilted and Torted Optic Discs among an Adult Chinese Population in Singapore: The Tanjong Pagar Study. Arch Ophthalmol 2009;127:894–9. - PubMed
-
- Vongphanit J, Mitchell P, Wang JJ. Population Prevalence of Tilted Optic Disks and the Relationship of This Sign to Refractive Error. Am J Ophthalmol 2002;133:679–85. - PubMed
-
- You QS, Xu L, Jonas JB. Tilted Optic Discs: The Beijing Eye Study. Eye (Lond) 2008;22:728–9. - PubMed
-
- Apple DJ, Rabb MF, Walsh PM. Congenital Anomalies of the Optic Disc. Surv Ophthalmol 1982;27:3–41. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
