

Beyond Low Tidal Volume Ventilation: Treatment Adjuncts for Severe Respiratory Failure in Acute Respiratory Distress Syndrome
- PMID: 30247273
- PMCID: PMC6277052
- DOI: 10.1097/CCM.0000000000003406
Beyond Low Tidal Volume Ventilation: Treatment Adjuncts for Severe Respiratory Failure in Acute Respiratory Distress Syndrome
Abstract
Objectives: Despite decades of research, the acute respiratory distress syndrome remains associated with significant morbidity and mortality. This Concise Definitive Review provides a practical and evidence-based summary of treatments in addition to low tidal volume ventilation and their role in the management of severe respiratory failure in acute respiratory distress syndrome.
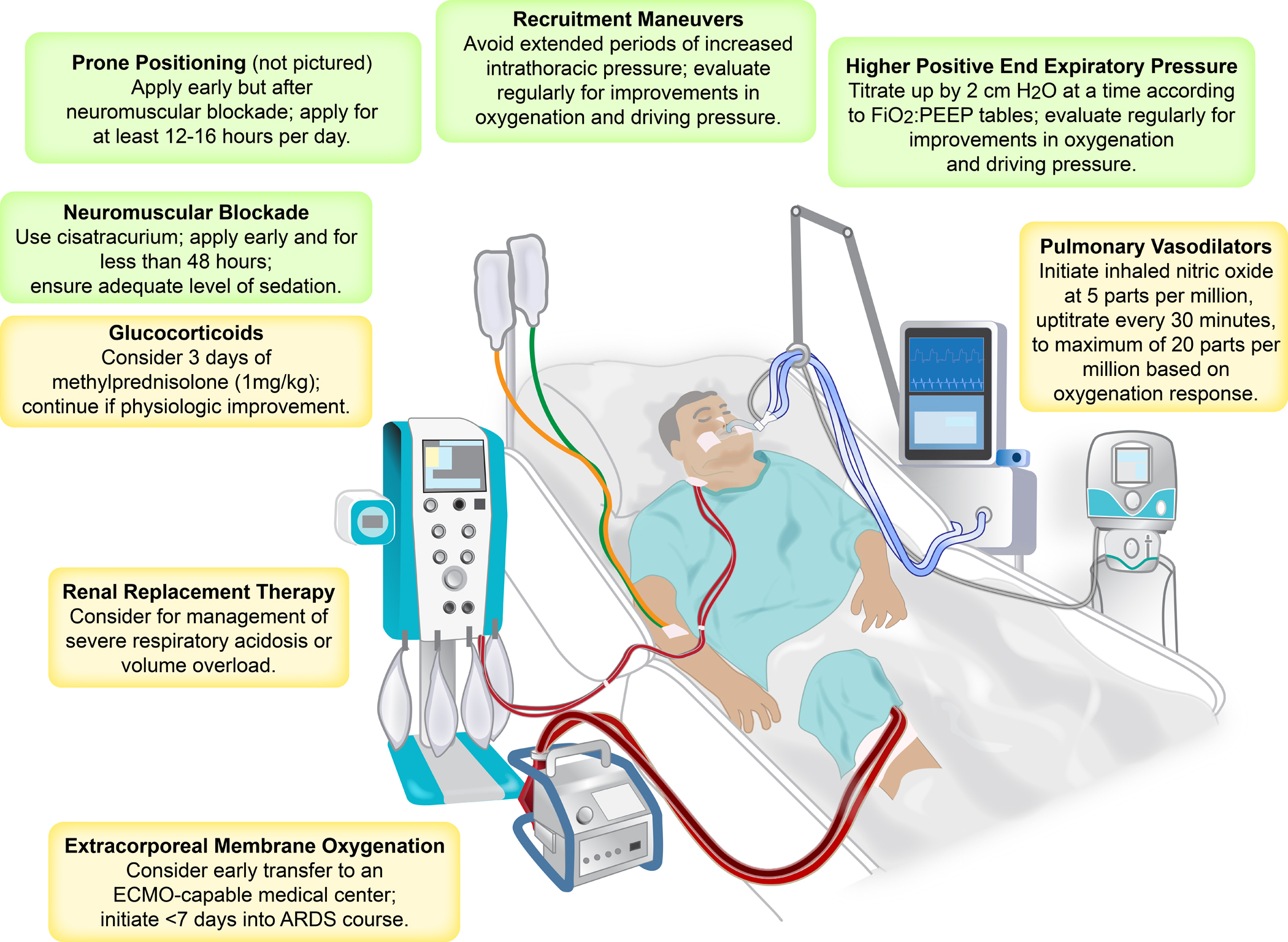
Data sources: We searched the PubMed database for clinical trials, observational studies, and review articles describing treatment adjuncts in acute respiratory distress syndrome patients, including high positive end-expiratory pressure strategies, recruitment maneuvers, high-frequency oscillatory ventilation, neuromuscular blockade, prone positioning, inhaled pulmonary vasodilators, extracorporeal membrane oxygenation, glucocorticoids, and renal replacement therapy.
Study selection and data extraction: Results were reviewed by the primary author in depth. Disputed findings and conclusions were then reviewed with the other authors until consensus was achieved.
Data synthesis: Severe respiratory failure in acute respiratory distress syndrome may present with refractory hypoxemia, severe respiratory acidosis, or elevated plateau airway pressures despite lung-protective ventilation according to acute respiratory distress syndrome Network protocol. For severe hypoxemia, first-line treatment adjuncts include high positive end-expiratory pressure strategies, recruitment maneuvers, neuromuscular blockade, and prone positioning. For refractory acidosis, we recommend initial modest liberalization of tidal volumes, followed by neuromuscular blockade and prone positioning. For elevated plateau airway pressures, we suggest first decreasing tidal volumes, followed by neuromuscular blockade, modification of positive end-expiratory pressure, and prone positioning. Therapies such as inhaled pulmonary vasodilators, glucocorticoids, and renal replacement therapy have significantly less evidence in favor of their use and should be considered second line. Extracorporeal membrane oxygenation may be life-saving in selected patients with severe acute respiratory distress syndrome but should be used only when other alternatives have been applied.
Conclusions: Severe respiratory failure in acute respiratory distress syndrome often necessitates the use of treatment adjuncts. Evidence-based application of these therapies in acute respiratory distress syndrome remains a significant challenge. However, a rational stepwise approach with frequent monitoring for improvement or harm can be achieved.
Conflict of interest statement
Figures
Comment in
-
Methylprednisolone: Likely an Effective Treatment in Acute Respiratory Distress Syndrome.Crit Care Med. 2019 Apr;47(4):e374-e375. doi: 10.1097/CCM.0000000000003572. Crit Care Med. 2019. PMID: 30882439 No abstract available.
-
The authors reply.Crit Care Med. 2019 Apr;47(4):e375-e376. doi: 10.1097/CCM.0000000000003648. Crit Care Med. 2019. PMID: 30882440 Free PMC article. No abstract available.
-
Airway Pressure Release Ventilation as a Rescue for Acute Respiratory Distress Syndrome But Use Early to Prevent It!Crit Care Med. 2019 Apr;47(4):e379-e380. doi: 10.1097/CCM.0000000000003594. Crit Care Med. 2019. PMID: 30882445 No abstract available.
-
The authors reply.Crit Care Med. 2019 Apr;47(4):e380-e381. doi: 10.1097/CCM.0000000000003666. Crit Care Med. 2019. PMID: 30882446 Free PMC article. No abstract available.
References
-
- Ashbaugh DG, Bigelow DB, Petty TL, Levine BE: Acute respiratory distress in adults. Lancet 1967, 2(7511):319–323. - PubMed
-
- Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, Gattinoni L, van Haren F, Larsson A, McAuley DF et al. : Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA 2016, 315(8):788–800. - PubMed
-
- Brower RG, Matthay MA, Morris A, Schoenfeld D, Thompson BT, Wheeler A: Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med 2000, 342(18):1301–1308. - PubMed
-
- Fan E, Del Sorbo L, Goligher EC, Hodgson CL, Munshi L, Walkey AJ, Adhikari NKJ, Amato MBP, Branson R, Brower RG et al. : An official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine clinical practice guideline: Mechanical ventilation in adult patients with acute respiratory distress syndrome. Am J Respir Crit Care Med 2017, 195(9):1253–1263. - PubMed
-
- Force ADT, Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E, Camporota L, Slutsky AS: Acute respiratory distress syndrome: The Berlin definition. JAMA 2012, 307(23):2526–2533. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
