

Using behaviour change theory and preliminary testing to develop an implementation intervention to reduce imaging for low back pain
- PMID: 30249241
- PMCID: PMC6154885
- DOI: 10.1186/s12913-018-3526-7
Using behaviour change theory and preliminary testing to develop an implementation intervention to reduce imaging for low back pain
Abstract
Background: Imaging is overused in the management of low back pain (LBP). Interventions designed to decrease non-indicated imaging have predominantly targeted practitioner education alone; however, these are typically ineffective. Barriers to reducing imaging have been identified for both patients and practitioners. Interventions aimed at addressing barriers in both these groups concurrently may be more effective. The Behaviour Change Wheel provides a structured framework for developing implementation interventions to facilitate behavioural change. The aim of this study was to develop an implementation intervention aiming to reduce non-indicated imaging for LBP, by targeting both general medical practitioner (GP) and patient barriers concurrently.
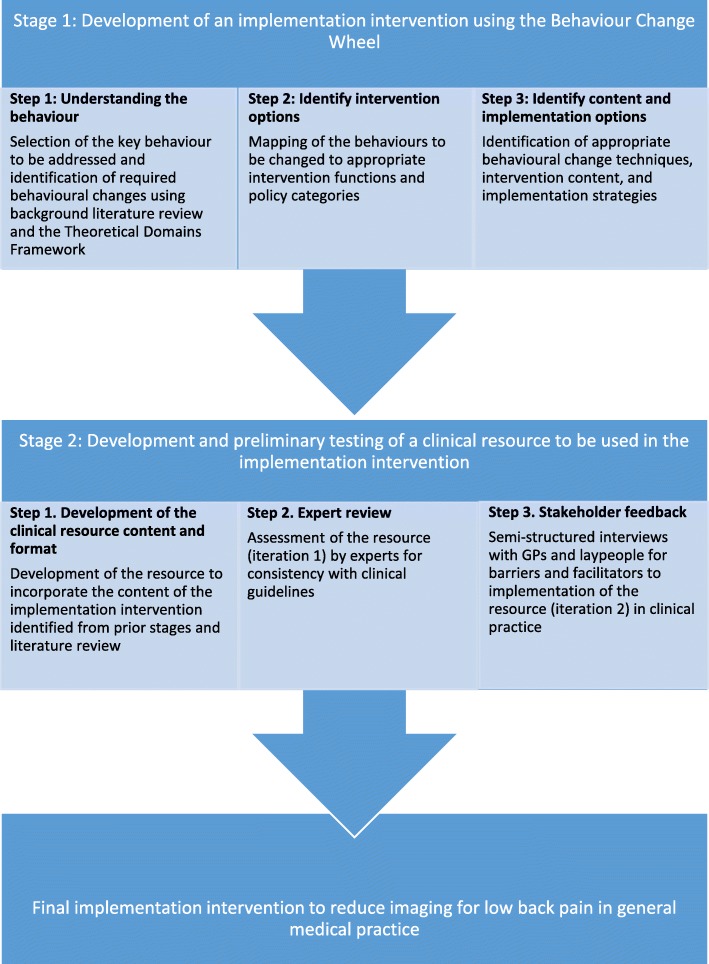
Methods: The Behaviour Change Wheel was used to identify the behaviours requiring change, and guide initial development of an implementation intervention. Preliminary testing of the intervention was performed with: 1) content review by experts in the field; and 2) qualitative analysis of semi-structured interviews with 10 GPs and 10 healthcare consumers, to determine barriers and facilitators to successful implementation of the intervention in clinical practice. Results informed further development of the implementation intervention.
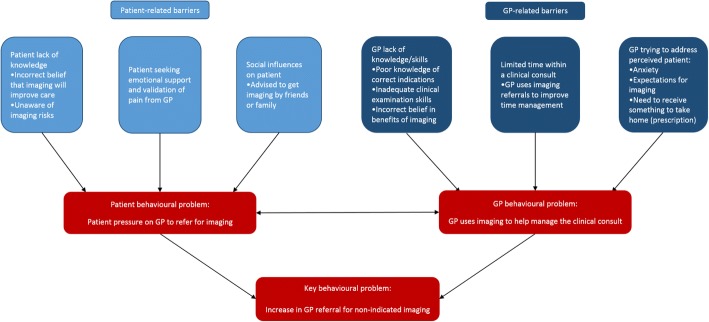
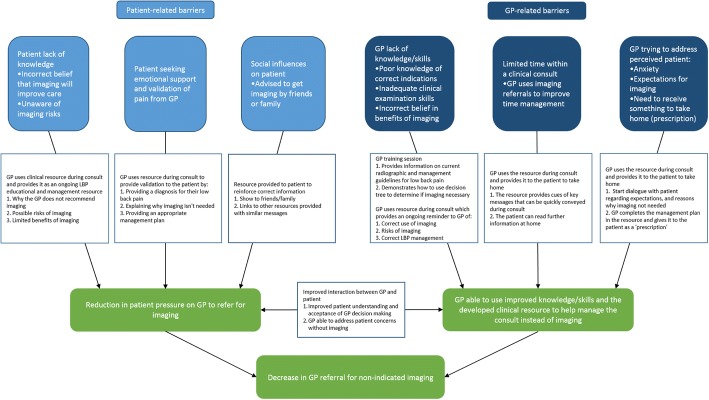
Results: Patient pressure on the GP to order imaging, and the inability of the GP to manage a clinical consult for LBP without imaging, were determined to be the primary behaviours leading to referral for non-indicated imaging. The developed implementation intervention consisted of a purpose-developed clinical resource for GPs to use with patients during a LBP consult, and a GP training session. The implementation intervention was designed to provide GP and patient education, remind GPs of preferred behaviour, provide clinical decision support, and facilitate GP-patient communication. Preliminary testing found experts, GPs, and healthcare consumers were supportive of most aspects of the developed resource, and thought use would likely decrease non-indicated imaging for LBP. Suggestions for improvement of the implementation intervention were incorporated into a final version.
Conclusions: The developed implementation intervention, aiming to reduce non-indicated imaging for LBP, was informed by behaviour change theory and preliminary testing. Further testing is required to assess feasibility of use in clinical practice, and the effectiveness of the implementation intervention in reducing imaging for LBP, before large-scale implementation can be considered.
Keywords: Behaviour change wheel; Diagnostic imaging; Intervention development; Low back pain, implementation intervention.
Conflict of interest statement
Ethics approval and consent to participate
Ethics approval was granted by Macquarie University Human Research Ethics Committee (MUHREC), reference number: 5201600298. All participants gave their consent and permission to participate in this study.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
General practitioner views on the determinants of test ordering: a theory-based qualitative approach to the development of an intervention to improve immunoglobulin requests in primary care.Implement Sci. 2016 Jul 19;11(1):102. doi: 10.1186/s13012-016-0465-8. Implement Sci. 2016. PMID: 27435839 Free PMC article.
-
Improving medication management in multimorbidity: development of the MultimorbiditY COllaborative Medication Review And DEcision Making (MY COMRADE) intervention using the Behaviour Change Wheel.Implement Sci. 2015 Sep 24;10:132. doi: 10.1186/s13012-015-0322-1. Implement Sci. 2015. PMID: 26404642 Free PMC article.
-
General practitioner experiences using a low back pain management booklet aiming to decrease non-indicated imaging for low back pain.Implement Sci Commun. 2022 Jun 28;3(1):71. doi: 10.1186/s43058-022-00317-y. Implement Sci Commun. 2022. PMID: 35765064 Free PMC article.
-
Physician-reported barriers to using evidence-based recommendations for low back pain in clinical practice: a systematic review and synthesis of qualitative studies using the Theoretical Domains Framework.Implement Sci. 2019 May 7;14(1):49. doi: 10.1186/s13012-019-0884-4. Implement Sci. 2019. PMID: 31064375 Free PMC article.
-
Effectiveness of Interventions to Decrease Image Ordering for Low Back Pain Presentations in the Emergency Department: A Systematic Review.Acad Emerg Med. 2018 Jun;25(6):614-626. doi: 10.1111/acem.13376. Epub 2018 Feb 19. Acad Emerg Med. 2018. PMID: 29315969
Cited by
-
Evaluation of a guidelines implementation intervention to reduce work disability and sick leaves related to chronic musculoskeletal pain: a theory-informed qualitative study in occupational health care.BMC Musculoskelet Disord. 2022 Mar 22;23(1):272. doi: 10.1186/s12891-022-05234-8. BMC Musculoskelet Disord. 2022. PMID: 35317760 Free PMC article.
-
Exploring factors influencing chiropractors' adherence to radiographic guidelines for low back pain using the Theoretical Domains Framework.Chiropr Man Therap. 2022 May 9;30(1):23. doi: 10.1186/s12998-022-00433-5. Chiropr Man Therap. 2022. PMID: 35534902 Free PMC article.
-
Patient and general practitioner views of tools to delay diagnostic imaging for low back pain: a qualitative study.BMJ Open. 2020 Nov 8;10(11):e039936. doi: 10.1136/bmjopen-2020-039936. BMJ Open. 2020. PMID: 33162393 Free PMC article.
-
Implementation interventions for musculoskeletal programs of care in the active military and barriers, facilitators, and outcomes of implementation: a scoping review.Implement Sci. 2019 Aug 16;14(1):82. doi: 10.1186/s13012-019-0931-1. Implement Sci. 2019. PMID: 31419992 Free PMC article.
-
Identifying and prioritizing do-not-do recommendations in Dutch primary care.BMC Prim Care. 2022 Jun 3;23(1):141. doi: 10.1186/s12875-022-01713-y. BMC Prim Care. 2022. PMID: 35658832 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
