

Cerebral influx of Na+ and Cl- as the osmotherapy-mediated rebound response in rats
- PMID: 30249273
- PMCID: PMC6154956
- DOI: 10.1186/s12987-018-0111-8
Cerebral influx of Na+ and Cl- as the osmotherapy-mediated rebound response in rats
Abstract
Background: Cerebral edema can cause life-threatening increase in intracranial pressure. Besides surgical craniectomy performed in severe cases, osmotherapy may be employed to lower the intracranial pressure by osmotic extraction of cerebral fluid upon intravenous infusion of mannitol or NaCl. A so-called rebound effect can, however, hinder continuous reduction in cerebral fluid by yet unresolved mechanisms.
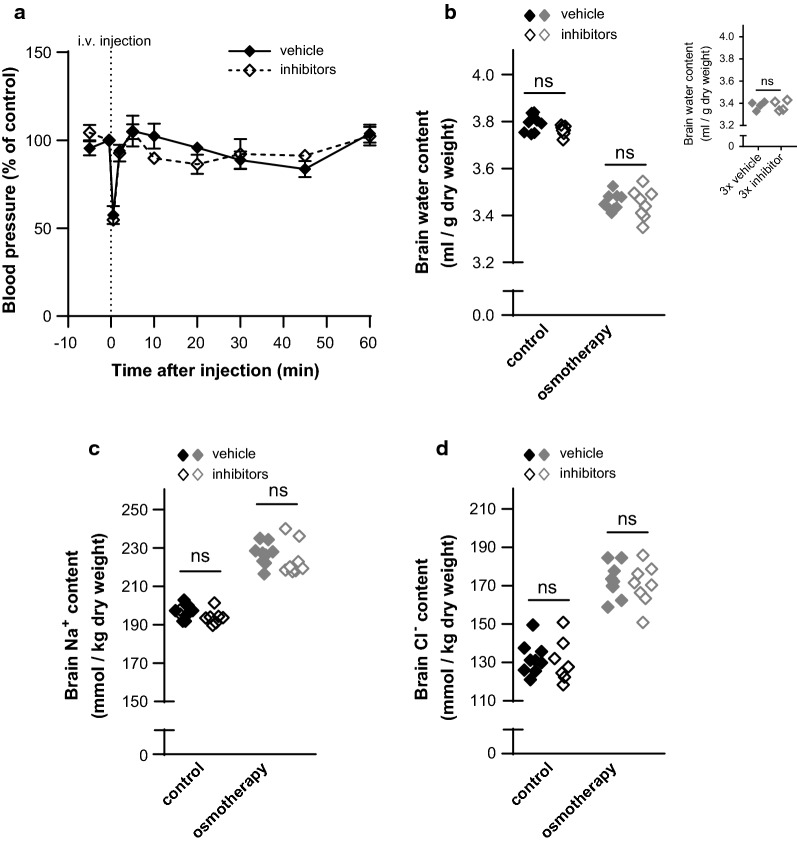
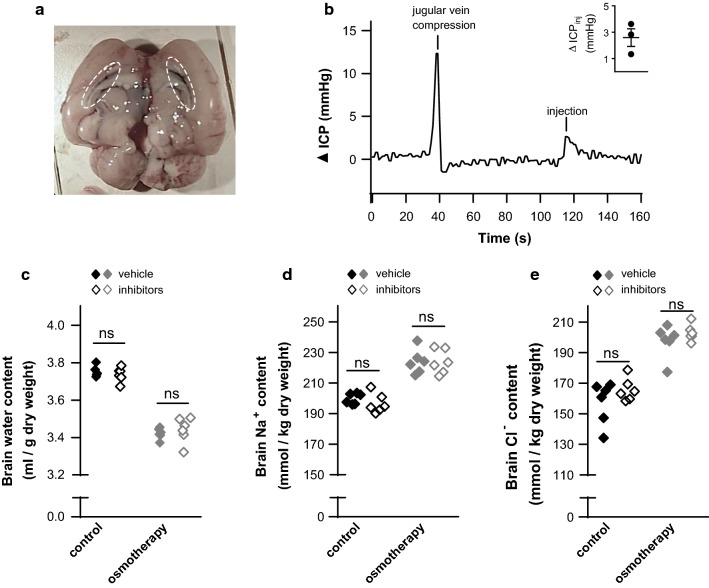
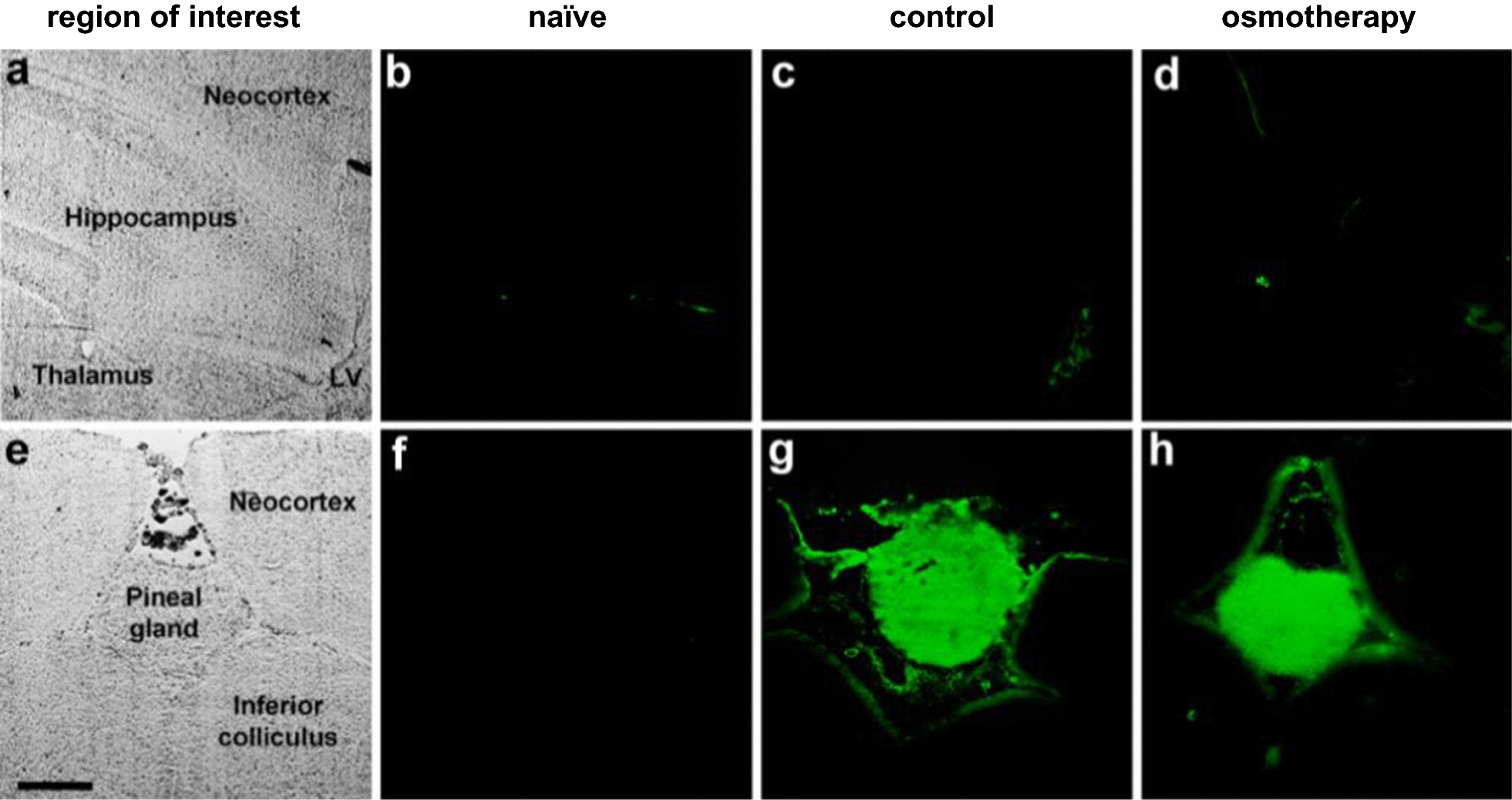
Methods: We determined the brain water and electrolyte content in healthy rats treated with osmotherapy. Osmotherapy (elevated plasma osmolarity) was mediated by intraperitoneal injection of NaCl or mannitol with inclusion of pharmacological inhibitors of selected ion-transporters present at the capillary lumen or choroidal membranes. Brain barrier integrity was determined by fluorescence detection following intravenous delivery of Na+-fluorescein.
Results: NaCl was slightly more efficient than mannitol as an osmotic agent. The brain water loss was only ~ 60% of that predicted from ideal osmotic behavior, which could be accounted for by cerebral Na+ and Cl- accumulation. This electrolyte accumulation represented the majority of the rebound response, which was unaffected by the employed pharmacological agents. The brain barriers remained intact during the elevated plasma osmolarity.
Conclusions: A brain volume regulatory response occurs during osmotherapy, leading to the rebound response. This response involves brain accumulation of Na+ and Cl- and takes place by unresolved molecular mechanisms that do not include the common ion-transporting mechanisms located in the capillary endothelium at the blood-brain barrier and in the choroid plexus epithelium at the blood-CSF barrier. Future identification of these ion-transporting routes could provide a pharmacological target to prevent the rebound effect associated with the widely used osmotherapy.
Keywords: Brain barriers; Brain edema; Ion-transporting mechanisms; Osmotherapy; Rebound effect.
Figures


References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
