

Care setting and 30-day hospital readmissions among older adults: a population-based cohort study
- PMID: 30249758
- PMCID: PMC6157496
- DOI: 10.1503/cmaj.180290
Care setting and 30-day hospital readmissions among older adults: a population-based cohort study
Abstract
Background: Despite the fact that many older adults receive home or long-term care services, the effect of these care settings on hospital readmission is often overlooked. Efforts to reduce hospital readmissions, including capacity planning and targeting of interventions, require clear data on the frequency of and risk factors for readmission among different populations of older adults.
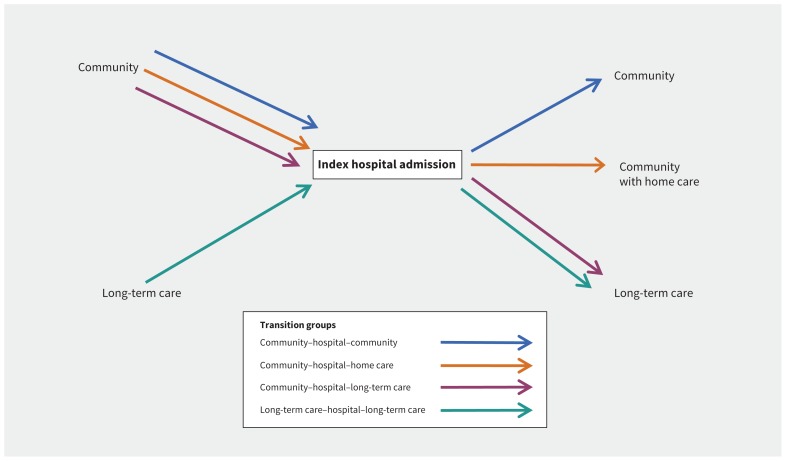
Methods: We identified all adults older than 65 years discharged from an unplanned medical hospital stay in Ontario between April 2008 and December 2015. We defined 2 preadmission care settings (community, long-term care) and 3 discharge care settings (community, home care, long-term care) and used multinomial regression to estimate associations with 30-day readmission (and death as a competing risk).
Results: We identified 701 527 individuals (mean age 78.4 yr), of whom 414 302 (59.1%) started in and returned to the community. Overall, 88 305 in dividuals (12.6%) were re admitted within 30 days, but this proportion varied by care setting combination. Relative to individuals returning to the community, those discharged to the community with home care (adjusted odds ratio [OR] 1.43, 95% confidence interval [CI] 1.39-1.46) and those returning to long-term care (adjusted OR 1.35, 95% CI 1.27-1.43) had a greater risk of readmission, whereas those newly admitted to long-term care had a lower risk of readmission (adjusted OR 0.68, 95% CI 0.63-0.72).
Interpretation: In Ontario, about 40% of older people were discharged from hospital to either home care or long-term care. These discharge settings, as well as whether an individual was admitted to hospital from long-term care, have important implications for understanding 30-day readmission rates. System planning and efforts to reduce readmission among older adults should take into account care settings at both admission and discharge.
© 2018 Joule Inc. or its licensors.
Conflict of interest statement
Competing interests: Chaim Bell is a medical consultant with the Policy and Innovations Branch of the Ontario Ministry of Health and Long-Term Care. No other competing interests were declared.
Figures
References
-
- Berenson RA, Paulus RA, Kalman NS. Medicare’s readmissions-reduction program — a positive alternative. N Engl J Med 2012;366:1364–6. - PubMed
-
- Dhalla IA, O’Brien T, Morra D, et al. Effect of a postdischarge virtual ward on readmission or death for high-risk patients. JAMA 2014;312:1305–12. - PubMed
-
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med 2009;360:1418–28. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous