

Association Between Type 2 Diabetes Mellitus, HbA1c and the Risk for Spontaneous Bacterial Peritonitis in Patients with Decompensated Liver Cirrhosis and Ascites
- PMID: 30250034
- PMCID: PMC6155293
- DOI: 10.1038/s41424-018-0053-0
Association Between Type 2 Diabetes Mellitus, HbA1c and the Risk for Spontaneous Bacterial Peritonitis in Patients with Decompensated Liver Cirrhosis and Ascites
Abstract
Introduction: Type 2 diabetes mellitus (DM) is a frequent comorbidity among patients with liver cirrhosis. However, data regarding the impact of DM on spontaneous bacterial peritonitis (SBP) are quite limited. Our aim was to analyze the impact of DM and HbA1c values on the incidence of SBP and mortality in patients with liver cirrhosis and ascites.
Methods: A number of 475 consecutive patients with liver cirrhosis and ascites were analyzed. Presence of DM as well as HbA1c was assessed at the time of the first paracentesis. Patients were followed up for a mean of 266 days. Primary endpoints were SBP development and mortality.
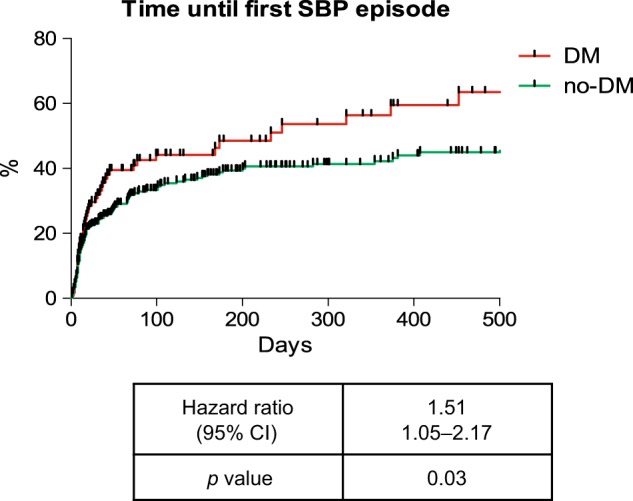
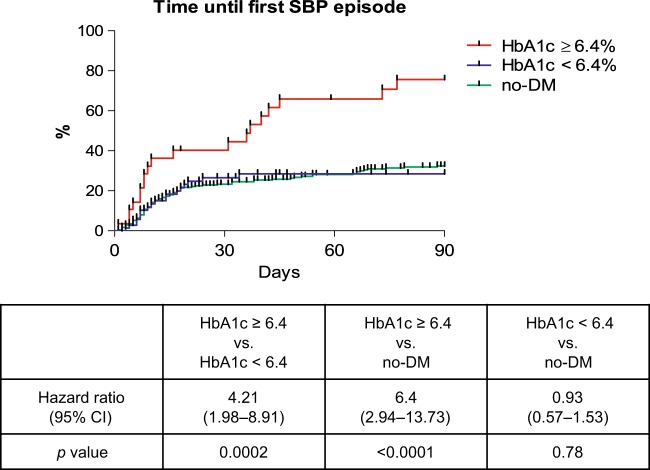
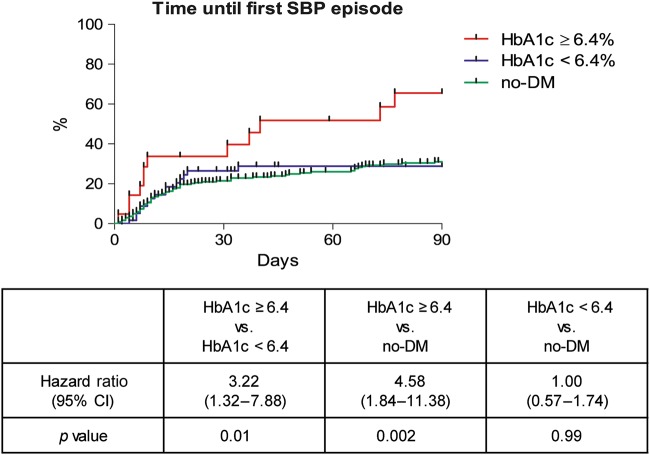
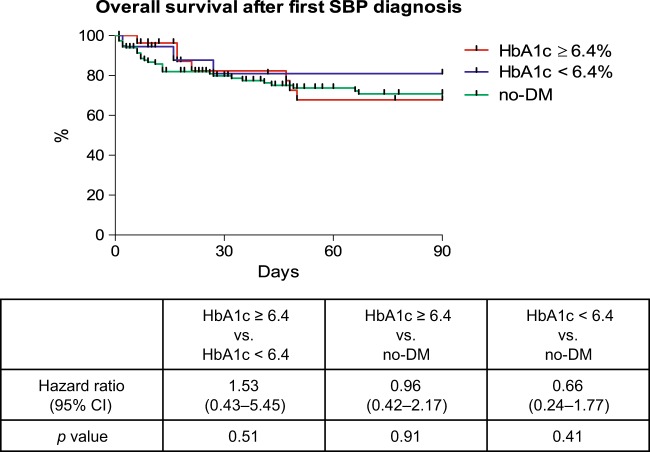
Results: Overall, 118 (25%) patients were diagnosed with DM. DM patients had an increased risk for developing a SBP during follow-up (HR: 1.51; p = 0.03). SBP incidence was particularly high in DM patients with HbA1c values ≥6.4%, significantly higher than in DM patients with HbA1c values <6.4% (HR: 4.21; p = 0.0002). Of note, DM patients with HbA1c <6.4% at baseline had a similar risk for SBP as those without DM (HR: 0.93; p = 0.78, respectively). After excluding all patients who were eligible for secondary antibiotic prophylaxis, HbA1c ≥6.4% but neither bilirubin nor ascites protein level were associated with primary SBP development in the multivariate analysis (p = 0.003).
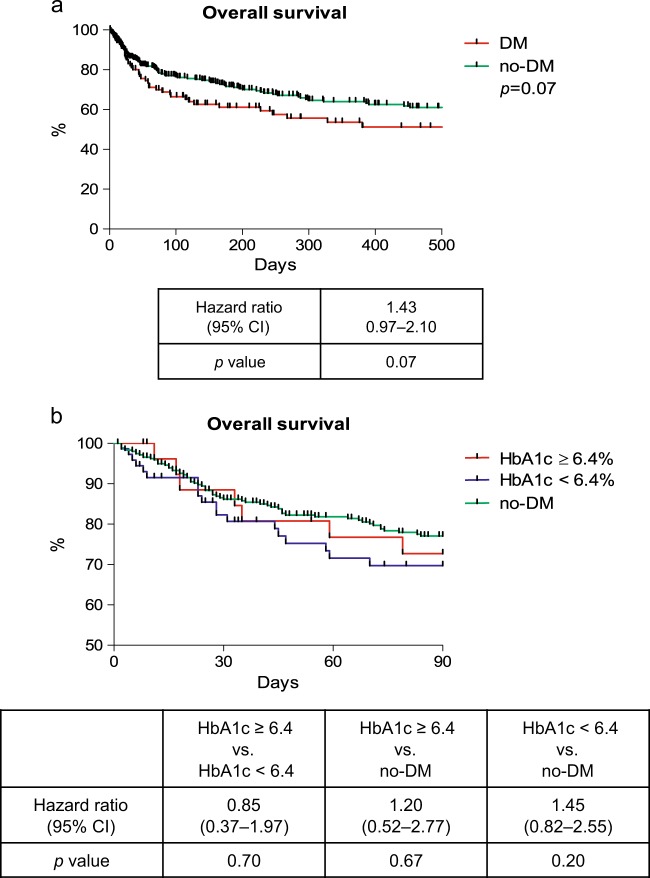
Conclusions: Individuals with liver cirrhosis and concomitant DM have a higher risk for developing a SBP. HbA1c values may be useful to further stratify the risk for SBP among DM patients, which may help to identify those who benefit from antibiotic prophylaxis.
Conflict of interest statement
Figures
Similar articles
-
Impact of rifaximin on the frequency and characteristics of spontaneous bacterial peritonitis in patients with liver cirrhosis and ascites.PLoS One. 2014 Apr 8;9(4):e93909. doi: 10.1371/journal.pone.0093909. eCollection 2014. PLoS One. 2014. PMID: 24714550 Free PMC article.
-
EVALUATION OF PROGNOSTIC FACTORS IN DECOMPENSATED LIVER CIRRHOSIS WITH ASCITES AND SPONTANEOUS BACTERIAL PERITONITIS.Rev Med Chir Soc Med Nat Iasi. 2015 Oct-Dec;119(4):1018-24. Rev Med Chir Soc Med Nat Iasi. 2015. PMID: 26793843
-
Risk factors for development of spontaneous bacterial peritonitis and subsequent mortality in cirrhotic patients with ascites.Liver Int. 2015 Sep;35(9):2121-8. doi: 10.1111/liv.12795. Epub 2015 Feb 18. Liver Int. 2015. PMID: 25644943
-
Spontaneous bacterial peritonitis. Detection, treatment and prophylaxis in patients with liver cirrhosis.Neth J Med. 1997 Oct;51(4):123-8. doi: 10.1016/s0300-2977(97)00042-9. Neth J Med. 1997. PMID: 9446921 Review.
-
Long-term prophylaxis of spontaneous bacterial peritonitis in patients with cirrhosis.Ann Pharmacother. 2005 May;39(5):908-12. doi: 10.1345/aph.1E585. Epub 2005 Mar 15. Ann Pharmacother. 2005. PMID: 15769829 Review.
Cited by
-
Sustained impact of nosocomial-acquired spontaneous bacterial peritonitis in different stages of decompensated liver cirrhosis.PLoS One. 2019 Aug 2;14(8):e0220666. doi: 10.1371/journal.pone.0220666. eCollection 2019. PLoS One. 2019. PMID: 31374111 Free PMC article.
-
Gut Microbiota and Infectious Complications in Advanced Chronic Liver Disease: Focus on Spontaneous Bacterial Peritonitis.Life (Basel). 2023 Apr 11;13(4):991. doi: 10.3390/life13040991. Life (Basel). 2023. PMID: 37109520 Free PMC article. Review.
-
Hepatogenous diabetes: Knowledge, evidence, and skepticism.World J Hepatol. 2022 Jul 27;14(7):1291-1306. doi: 10.4254/wjh.v14.i7.1291. World J Hepatol. 2022. PMID: 36158904 Free PMC article. Review.
-
Safety and feasibility of transjugular intrahepatic portosystemic shunt in elderly patients with liver cirrhosis and refractory ascites.PLoS One. 2020 Jun 25;15(6):e0235199. doi: 10.1371/journal.pone.0235199. eCollection 2020. PLoS One. 2020. PMID: 32584874 Free PMC article. Clinical Trial.
-
Diabetes mellitus and the risk of spontaneous bacterial peritonitis in patients with liver cirrhosis: a systematic review and meta-analysis.Ann Saudi Med. 2024 Jul-Aug;44(4):272-287. doi: 10.5144/0256-4947.2024.272. Epub 2024 Aug 1. Ann Saudi Med. 2024. PMID: 39127903 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
