

Intrapancreatic accessory spleen: Evaluation with CT and MRI
- PMID: 30250526
- PMCID: PMC6144032
- DOI: 10.3892/etm.2018.6613
Intrapancreatic accessory spleen: Evaluation with CT and MRI
Abstract
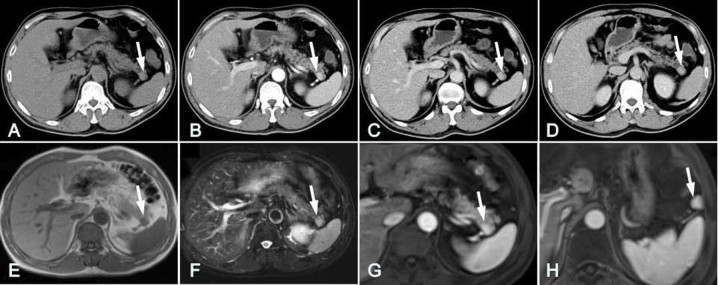
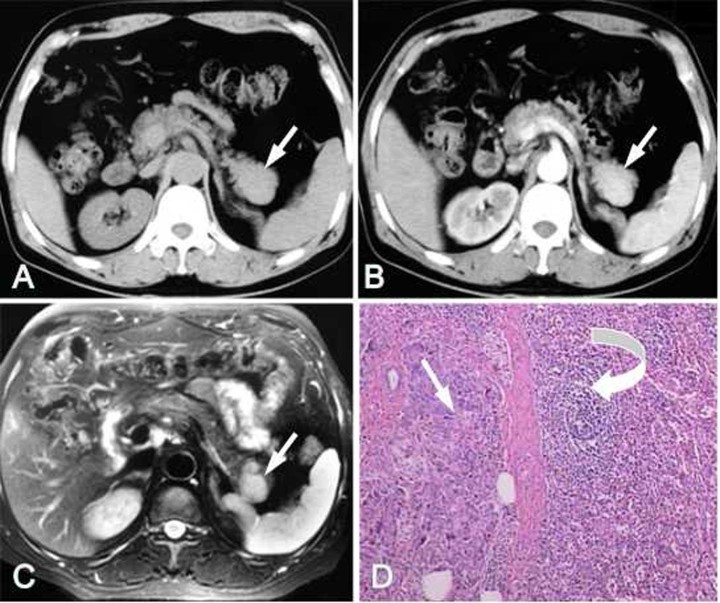
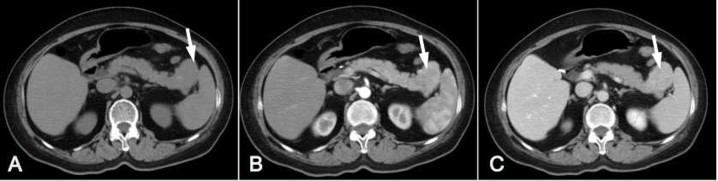
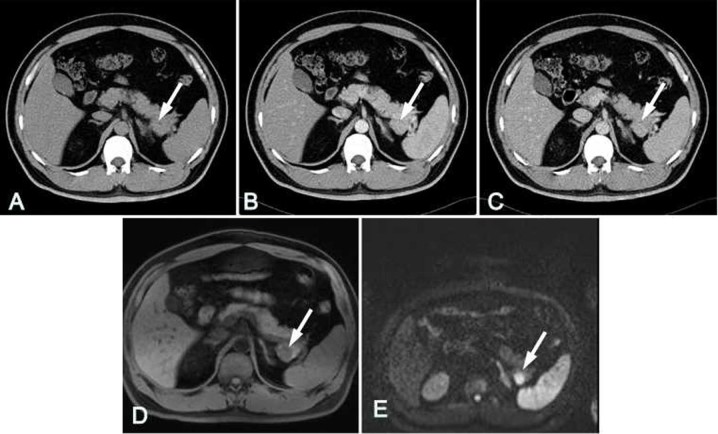
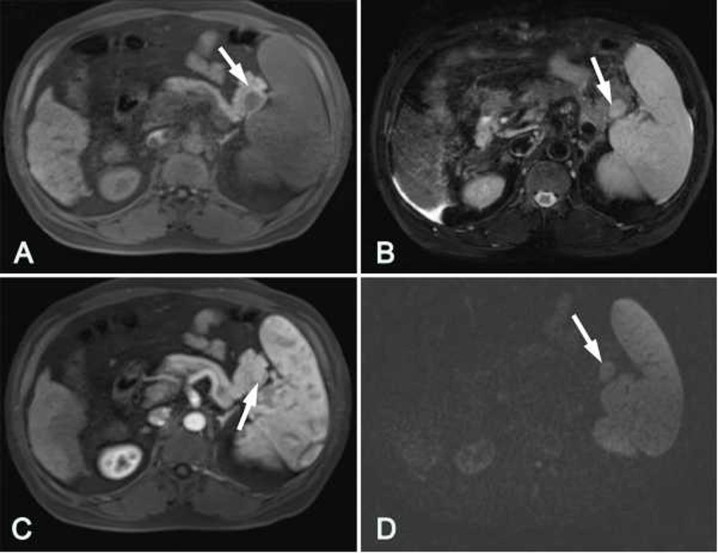
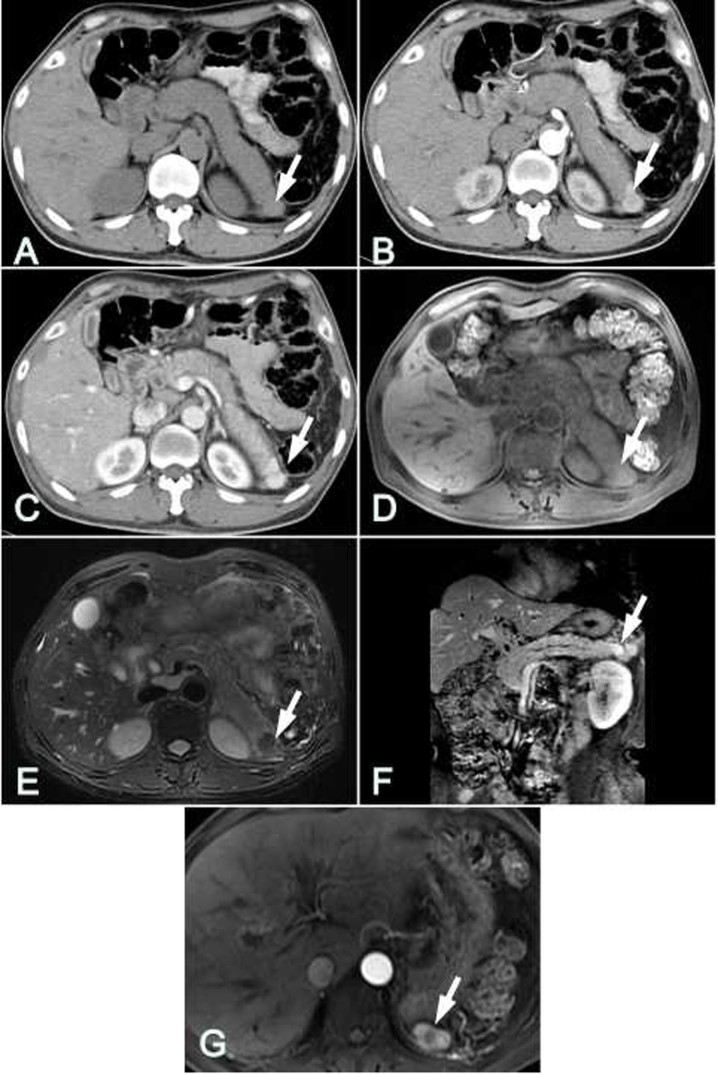
The aim of the present study was to evaluate the characteristics of computed tomography (CT) and magnetic resonance imaging (MRI), particularly diffusion-weighted imaging (DWI), in the imaging of intrapancreatic accessory spleen (IPAS). The clinical and pathological records of 9 patients, including 8 patients with IPAS and 1 patient with splenosis, were reviewed. The patients had undergone plain and triple-phase enhanced CT scanning (n=9) and MRI scanning (n=8). The lesions of the 8 IPAS patients were located in the pancreatic tail, and were round (n=3), oval (n=4) or triangular (n=1) in shape. The CT and/or MRI densities, signal intensities and dynamic enhanced patterns of the lesions were similar to those of the orthotopic spleen. In DWI images (n=5), the IPAS regions presented high signal intensity (SI), and no significant difference in the apparent diffusion coefficient determined using a b-value of 600 sec/mm2 was identified between the IPAS and orthotopic spleen (P>0.05). One patient with splenosis complicated with cirrhosis had a nodule located in the pancreatic tail with an unenhanced CT value of 65 HU. In MRI examination, with the exception of the dynamic enhancement pattern, the T1-weighted, T2-weighted and DWI signals of splenosis were inconsistent with those of the normal spleen. In conclusion, in pre-contrast and post-contrast-enhanced CT and MRI images, IPAS exhibits similar characteristics to the orthotopic spleen. CT and MRI used in combination with DWI are important in the diagnosis of IPAS.
Keywords: computed tomography; diffusion-weighted imaging; intrapancreatic accessory spleen; magnetic resonance imaging.
Figures

Similar articles
-
Significance of imaging findings in the diagnosis of heterotopic spleen-an intrapancreatic accessory spleen (IPAS): Case report.Medicine (Baltimore). 2017 Dec;96(52):e9040. doi: 10.1097/MD.0000000000009040. Medicine (Baltimore). 2017. PMID: 29384897 Free PMC article.
-
Diffusion-weighted MRI: usefulness for differentiating intrapancreatic accessory spleen and small hypervascular neuroendocrine tumor of the pancreas.Acta Radiol. 2014 Dec;55(10):1157-65. doi: 10.1177/0284185113513760. Epub 2013 Nov 20. Acta Radiol. 2014. PMID: 24259300
-
MDCT and superparamagnetic iron oxide (SPIO)-enhanced MR findings of intrapancreatic accessory spleen in seven patients.Eur Radiol. 2006 Sep;16(9):1887-97. doi: 10.1007/s00330-006-0193-6. Epub 2006 Mar 18. Eur Radiol. 2006. PMID: 16547707
-
Intrapancreatic accessory spleen: findings on MR Imaging, CT, US and scintigraphy, and the pathologic analysis.Korean J Radiol. 2008 Mar-Apr;9(2):162-74. doi: 10.3348/kjr.2008.9.2.162. Korean J Radiol. 2008. PMID: 18385564 Free PMC article. Review.
-
Intrapancreatic accessory spleen: CT appearance and differential diagnosis.Abdom Imaging. 2012 Oct;37(5):812-27. doi: 10.1007/s00261-011-9830-x. Abdom Imaging. 2012. PMID: 22160284 Review.
Cited by
-
Accessory Spleen Masquerading as an Intrapancreatic Tumor: A Case Report.Cureus. 2022 May 2;14(5):e24677. doi: 10.7759/cureus.24677. eCollection 2022 May. Cureus. 2022. PMID: 35663712 Free PMC article.
-
Intrapancreatic accessory spleen: An imaging enigma.Indian J Radiol Imaging. 2020 Jul-Sep;30(3):392-394. doi: 10.4103/ijri.IJRI_407_20. Epub 2020 Oct 15. Indian J Radiol Imaging. 2020. PMID: 33273778 Free PMC article.
-
Differentiation of intrapancreatic accessory spleen from pancreatic neuroendocrine tumor using MRI R2.Abdom Radiol (NY). 2025 Aug;50(8):3674-3684. doi: 10.1007/s00261-024-04758-y. Epub 2025 Jan 22. Abdom Radiol (NY). 2025. PMID: 39841231
-
Rare Solid Pancreatic Lesions on Cross-Sectional Imaging.Diagnostics (Basel). 2023 Aug 21;13(16):2719. doi: 10.3390/diagnostics13162719. Diagnostics (Basel). 2023. PMID: 37627978 Free PMC article. Review.
-
Challenging Diagnosis of Intrapancreatic Accessory Spleen in the Tail of the Pancreas: A Case Report.Am J Case Rep. 2023 May 12;24:e939324. doi: 10.12659/AJCR.939324. Am J Case Rep. 2023. PMID: 37170482 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources