

Navigating Systemic Therapy in Advanced Thyroid Carcinoma: From Standard of Care to Personalized Therapy and Beyond
- PMID: 30250937
- PMCID: PMC6141902
- DOI: 10.1210/js.2018-00180
Navigating Systemic Therapy in Advanced Thyroid Carcinoma: From Standard of Care to Personalized Therapy and Beyond
Abstract
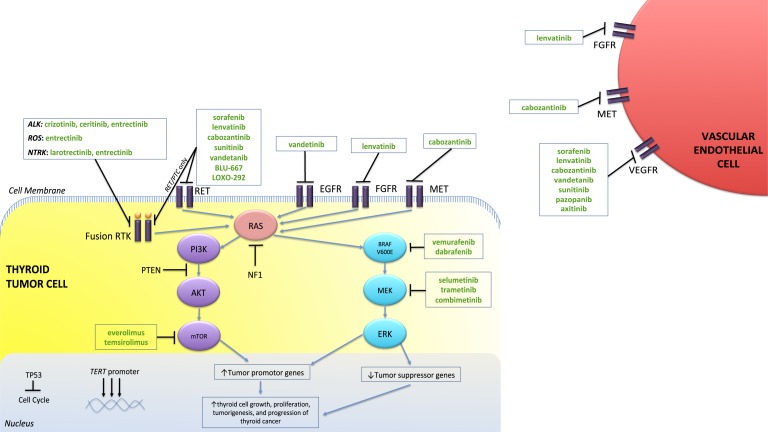
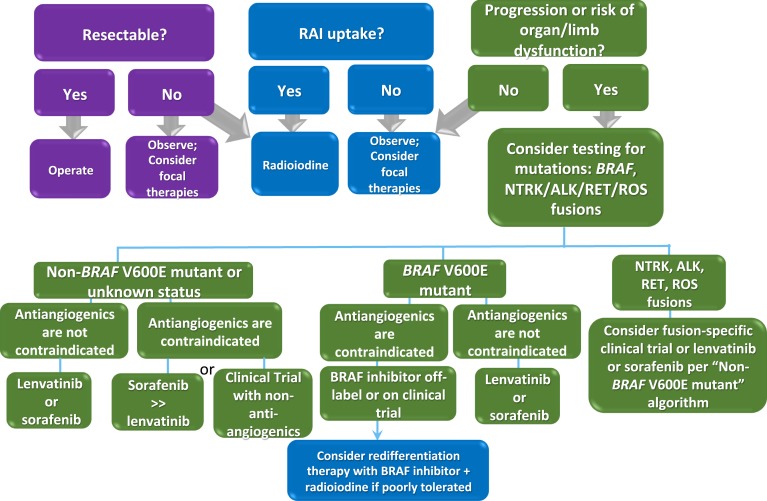
Thyroid cancer, with the exception of anaplastic thyroid cancer, typically has very favorable outcomes with the standard therapy. However, those that persist, recur, or metastasize are associated with a worse prognosis. Targeted therapy with kinase inhibitors has shown promise in advanced cases of thyroid cancer, and currently five drug regimens are approved for use in clinical practice in the treatment of differentiated, medullary, and anaplastic thyroid cancer, with more options in the pipeline. However, one of the greatest dilemmas is when and how to initiate one of these drugs, and this is discussed herein.
Keywords: BRAF inhibitors; anaplastic thyroid cancer; differentiated thyroid cancer; immunotherapy; kinase inhibitors; medullary thyroid cancer.
Figures
Similar articles
-
Perspectives on the Treatment of Advanced Thyroid Cancer: Approved Therapies, Resistance Mechanisms, and Future Directions.Front Oncol. 2021 Jan 25;10:592202. doi: 10.3389/fonc.2020.592202. eCollection 2020. Front Oncol. 2021. PMID: 33569345 Free PMC article. Review.
-
Targeted Therapy in Thyroid Cancer: State of the Art.Clin Oncol (R Coll Radiol). 2017 May;29(5):316-324. doi: 10.1016/j.clon.2017.02.009. Epub 2017 Mar 17. Clin Oncol (R Coll Radiol). 2017. PMID: 28318881 Review.
-
Clinical and Translational Challenges in Thyroid Cancer.Curr Med Chem. 2020;27(29):4806-4822. doi: 10.2174/0929867327666200214125712. Curr Med Chem. 2020. PMID: 32056516 Review.
-
Novel targeted therapies and immunotherapy for advanced thyroid cancers.Mol Cancer. 2018 Feb 19;17(1):51. doi: 10.1186/s12943-018-0786-0. Mol Cancer. 2018. PMID: 29455653 Free PMC article. Review.
-
Personalized therapy in patients with anaplastic thyroid cancer: targeting genetic and epigenetic alterations.J Clin Endocrinol Metab. 2015 Jan;100(1):35-42. doi: 10.1210/jc.2014-2803. J Clin Endocrinol Metab. 2015. PMID: 25347569 Free PMC article. Review.
Cited by
-
Metastatic medullary thyroid carcinoma: a new way forward.Endocr Relat Cancer. 2022 May 31;29(7):R85-R103. doi: 10.1530/ERC-21-0368. Endocr Relat Cancer. 2022. PMID: 35521769 Free PMC article. Review.
-
miR-590-5p mediates mitochondrial respiration, proliferation, and apoptosis in thyroid carcinoma cells via fibroblast growth factor receptor substrate 2.Arch Endocrinol Metab. 2025 Aug 20;69(4):e240410. doi: 10.20945/2359-4292-2024-0410. Arch Endocrinol Metab. 2025. PMID: 40834280 Free PMC article.
-
Analytical and Clinical Validation of Expressed Variants and Fusions From the Whole Transcriptome of Thyroid FNA Samples.Front Endocrinol (Lausanne). 2019 Sep 11;10:612. doi: 10.3389/fendo.2019.00612. eCollection 2019. Front Endocrinol (Lausanne). 2019. PMID: 31572297 Free PMC article.
-
Medullary Thyroid Cancer - Feature Review and Update on Systemic Treatment.Acta Clin Croat. 2020 Jun;59(Suppl 1):50-59. doi: 10.20471/acc.2020.59.s1.06. Acta Clin Croat. 2020. PMID: 34219884 Free PMC article. Review.
-
New approaches for patients with advanced radioiodine-refractory thyroid cancer.World J Clin Oncol. 2022 Jan 24;13(1):9-27. doi: 10.5306/wjco.v13.i1.9. World J Clin Oncol. 2022. PMID: 35116229 Free PMC article. Review.
References
-
- Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin. 2014;64(1):9–29. - PubMed
-
- Tuttle RM, Ball DW, Byrd D, Dilawari RA, Doherty GM, Duh QY, Ehya H, Farrar WB, Haddad RI, Kandeel F, Kloos RT, Kopp P, Lamonica DM, Loree TR, Lydiatt WM, McCaffrey JC, Olson JA Jr, Parks L, Ridge JA, Shah JP, Sherman SI, Sturgeon C, Waguespack SG, Wang TN, Wirth LJ; National Comprehensive Cancer Network . Thyroid carcinoma. J Natl Compr Canc Netw. 2010;8(11):1228–1274. - PubMed
-
- Elisei R, Molinaro E, Agate L, Bottici V, Masserini L, Ceccarelli C, Lippi F, Grasso L, Basolo F, Bevilacqua G, Miccoli P, Di Coscio G, Vitti P, Pacini F, Pinchera A. Are the clinical and pathological features of differentiated thyroid carcinoma really changed over the last 35 years? Study on 4187 patients from a single Italian institution to answer this question. J Clin Endocrinol Metab. 2010;95(4):1516–1527. - PubMed
-
- Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, Pacini F, Randolph GW, Sawka AM, Schlumberger M, Schuff KG, Sherman SI, Sosa JA, Steward DL, Tuttle RM, Wartofsky L. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2016;26(1):1–133. - PMC - PubMed
-
- Durante C, Haddy N, Baudin E, Leboulleux S, Hartl D, Travagli JP, Caillou B, Ricard M, Lumbroso JD, De Vathaire F, Schlumberger M. Long-term outcome of 444 patients with distant metastases from papillary and follicular thyroid carcinoma: benefits and limits of radioiodine therapy. J Clin Endocrinol Metab. 2006;91(8):2892–2899. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials