

Artificial Pancreas or Novel Beta-Cell Replacement Therapies: a Race for Optimal Glycemic Control?
- PMID: 30250968
- PMCID: PMC6153567
- DOI: 10.1007/s11892-018-1073-6
Artificial Pancreas or Novel Beta-Cell Replacement Therapies: a Race for Optimal Glycemic Control?
Abstract
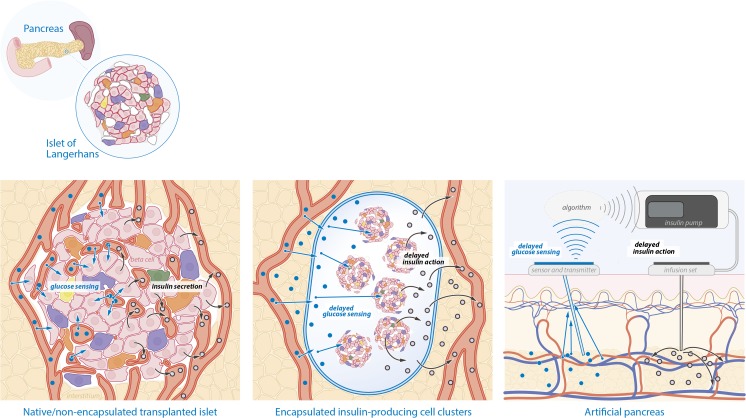
Purpose of review: New treatment strategies are needed for patients with type 1 diabetes (T1D). Closed loop insulin delivery and beta-cell replacement therapy are promising new strategies. This review aims to give an insight in the most relevant literature on this topic and to compare the two radically different treatment modalities.
Recent findings: Multiple clinical studies have been performed with closed loop insulin delivery devices and have shown an improvement in overall glycemic control and time spent in hypoglycemia. Beta-cell transplantation has been shown to normalize or greatly improve glycemic control in T1D, but the donor organ shortage and the necessity to use immunosuppressive agents are major drawbacks. Donor organ shortage may be solved by the utilization of stem cell-derived beta cells, which has shown great promise in animal models and are now tested in clinical studies. Immunosuppression may be avoided by encapsulation. Closed loop insulin delivery devices are promising treatment strategies and are likely to be used in clinical practice in the short term. But this approach will always suffer from delays in glucose measurement and insulin action preventing it from normalizing glycemic control. In the long term, stem cell-derived beta cell transplantation may be able to achieve this, but wide implementation in clinical practice is still far away.
Keywords: Bionic pancreas; Diabetes mellitus; Stem cells.
Conflict of interest statement
Conflict of Interest
Michiel F. Nijhoff and Eelco J.P. de Koning declare that they have no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Figures
Similar articles
-
Current topics in glycemic control by wearable artificial pancreas or bedside artificial pancreas with closed-loop system.J Artif Organs. 2016 Sep;19(3):209-18. doi: 10.1007/s10047-016-0904-y. Epub 2016 May 3. J Artif Organs. 2016. PMID: 27142278 Review.
-
Lessons from Human Islet Transplantation Inform Stem Cell-Based Approaches in the Treatment of Diabetes.Front Endocrinol (Lausanne). 2021 Mar 11;12:636824. doi: 10.3389/fendo.2021.636824. eCollection 2021. Front Endocrinol (Lausanne). 2021. PMID: 33776933 Free PMC article. Review.
-
Navigating Two Roads to Glucose Normalization in Diabetes: Automated Insulin Delivery Devices and Cell Therapy.Cell Metab. 2019 Mar 5;29(3):545-563. doi: 10.1016/j.cmet.2019.02.007. Cell Metab. 2019. PMID: 30840911 Review.
-
Differentiation and transplantation of functional pancreatic beta cells generated from induced pluripotent stem cells derived from a type 1 diabetes mouse model.Stem Cells Dev. 2012 Sep 20;21(14):2642-55. doi: 10.1089/scd.2011.0665. Epub 2012 Jun 1. Stem Cells Dev. 2012. PMID: 22512788 Free PMC article.
-
In vitro generation of pancreatic β-cells for diabetes treatment. I. β-like cells derived from human pluripotent stem cells.Folia Histochem Cytobiol. 2019;57(1):1-14. doi: 10.5603/FHC.a2019.0001. Epub 2019 Mar 14. Folia Histochem Cytobiol. 2019. PMID: 30869153 Review.
Cited by
-
Translational Research Symposium-collaborative efforts as driving forces of healthcare innovation.J Mater Sci Mater Med. 2019 Dec 2;30(12):133. doi: 10.1007/s10856-019-6339-2. J Mater Sci Mater Med. 2019. PMID: 31792698
-
The Role of Interleukin-1β in Destruction of Transplanted Islets.Cell Transplant. 2020 Jan-Dec;29:963689720934413. doi: 10.1177/0963689720934413. Cell Transplant. 2020. PMID: 32543895 Free PMC article. Review.
-
Stem Cell Transplantation in the Treatment of Type 1 Diabetes Mellitus: From Insulin Replacement to Beta-Cell Replacement.Front Endocrinol (Lausanne). 2022 Mar 18;13:859638. doi: 10.3389/fendo.2022.859638. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 35370989 Free PMC article. Review.
-
Engineering the vasculature for islet transplantation.Acta Biomater. 2019 Sep 1;95:131-151. doi: 10.1016/j.actbio.2019.05.051. Epub 2019 May 23. Acta Biomater. 2019. PMID: 31128322 Free PMC article. Review.
-
Impact of a Public Health Emergency on Behavior, Stress, Anxiety and Glycemic Control in Patients With Pancreas or Islet Transplantation for Type 1 Diabetes.Transpl Int. 2024 Mar 27;37:12278. doi: 10.3389/ti.2024.12278. eCollection 2024. Transpl Int. 2024. PMID: 38601276 Free PMC article. Clinical Trial.
References
-
- World Health Organization (2016) Global Report on Diabetes. http://apps.who.int/iris/bitstream/handle/10665/204871/9789241565257_eng... (Accessed april 2018).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
