

Association Between Subclinical Brain Infarcts and Functional Decline Trajectories
- PMID: 30251251
- PMCID: PMC6235693
- DOI: 10.1111/jgs.15557
Association Between Subclinical Brain Infarcts and Functional Decline Trajectories
Abstract
Objectives: To test associations between subclinical brain infarcts (SBIs) and functional decline independently of intervening clinical vascular events and other vascular risk factors.
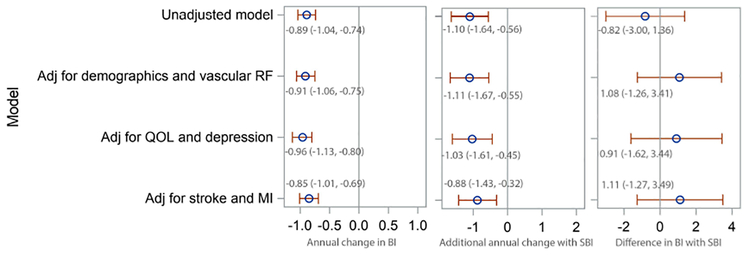
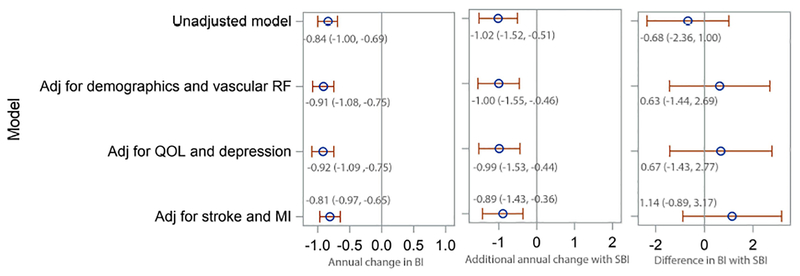
Design: Longitudinal follow-up for a mean 7.3 years. Generalized estimating equation models were used to test associations between SBIs, number of perivascular spaces (PVSs), baseline Barthel Index (BI), and change in BI, adjusting for sociodemographic, vascular, and cognitive risk factors and for stroke and myocardial infarction occurring during follow-up.
Setting: Population-based prospective cohort study.
Participants: Stroke-free individuals from the racially and ethnically diverse Northern Manhattan Study (N=1,290).
Measurements: Annual functional assessments using the BI (range 0-100).
Results: Mean age was 70.6 ± 9.0, 40% of participants were male, 66% were Hispanic, 193 (16%) had SBIs, and 508 (42%) had large PVSs. SBIs were not associated with baseline BI. In a fully adjusted model, there was a change in BI of -0.85 points per year (95% confidence interval (CI)=-1.01 to -0.69); those with SBI had an additional change in BI 0f -0.88 points (95% CI=-1.43 to -0.32). There were no associations between PVS and baseline BI or change in BI.
Conclusion: In a large population-based study, we found a strong and independent association between "subclinical" markers of cerebrovascular injury and important clinical, person-centered functional trajectories. Future research could clarify the evolution of such subclinical markers over time and test strategies to prevent their progression and minimize related disability. J Am Geriatr Soc 66:2144-2150, 2018.
Keywords: disability; epidemiology; subclinical brain infarct.
© 2018, Copyright the Authors Journal compilation © 2018, The American Geriatrics Society.
Conflict of interest statement
Figures
Similar articles
-
Cerebral white matter disease and functional decline in older adults from the Northern Manhattan Study: A longitudinal cohort study.PLoS Med. 2018 Mar 20;15(3):e1002529. doi: 10.1371/journal.pmed.1002529. eCollection 2018 Mar. PLoS Med. 2018. PMID: 29558467 Free PMC article.
-
Functional Trajectories, Cognition, and Subclinical Cerebrovascular Disease.Stroke. 2018 Mar;49(3):549-555. doi: 10.1161/STROKEAHA.117.019595. Epub 2018 Jan 26. Stroke. 2018. PMID: 29374104 Free PMC article. Clinical Trial.
-
Multiple Silent Brain Infarcts Are Associated with Severer Stroke in Patients with First-Ever Ischemic Stroke without Advanced Leukoaraiosis.J Stroke Cerebrovasc Dis. 2017 Sep;26(9):1988-1995. doi: 10.1016/j.jstrokecerebrovasdis.2017.06.011. Epub 2017 Jul 5. J Stroke Cerebrovasc Dis. 2017. PMID: 28688715
-
C-reactive protein is associated with disability independently of vascular events: the Northern Manhattan Study.Age Ageing. 2017 Jan 15;46(1):77-83. doi: 10.1093/ageing/afw179. Age Ageing. 2017. PMID: 28181636 Free PMC article.
-
Clinical Significance of Magnetic Resonance Imaging Markers of Vascular Brain Injury: A Systematic Review and Meta-analysis.JAMA Neurol. 2019 Jan 1;76(1):81-94. doi: 10.1001/jamaneurol.2018.3122. JAMA Neurol. 2019. PMID: 30422209 Free PMC article.
Cited by
-
Vascular Cognitive Impairment (VCI).Neurotherapeutics. 2022 Jan;19(1):68-88. doi: 10.1007/s13311-021-01170-y. Epub 2021 Dec 22. Neurotherapeutics. 2022. PMID: 34939171 Free PMC article. Review.
-
Intracranial artery stenosis is associated with cortical thinning in stroke-free individuals of two longitudinal cohorts.J Neurol Sci. 2023 Jan 15;444:120533. doi: 10.1016/j.jns.2022.120533. Epub 2022 Dec 23. J Neurol Sci. 2023. PMID: 36577280 Free PMC article.
References
-
- Vermeer SE, Longstreth WT Jr., Koudstaal PJ. Silent brain infarcts: A systematic review. Lancet Neurol. 2007;6:611–619 - PubMed
-
- Kim GM, Park KY, Avery R, Helenius J, Rost N, Rosand J, et al. Extensive leukoaraiosis is associated with high early risk of recurrence after ischemic stroke. Stroke. 2014;45:479–485 - PubMed
-
- Kuller LH, Arnold AM, Longstreth WT Jr., Manolio TA, O’Leary DH, Burke GL, et al. White matter grade and ventricular volume on brain mri as markers of longevity in the cardiovascular health study. Neurobiol Aging. 2007;28:1307–1315 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
