

Birth weight and cardiac function assessed by echocardiography in adolescence: Avon Longitudinal Study of Parents and Children
- PMID: 30251286
- PMCID: PMC6771817
- DOI: 10.1002/uog.20128
Birth weight and cardiac function assessed by echocardiography in adolescence: Avon Longitudinal Study of Parents and Children
Abstract
Objective: Maternal hemodynamics in pregnancy is associated with fetal growth and birth weight, which in turn are associated with offspring cardiovascular disease later in life. The aim of this study was to quantify the extent to which birth weight is associated with cardiac structure and function in adolescence.
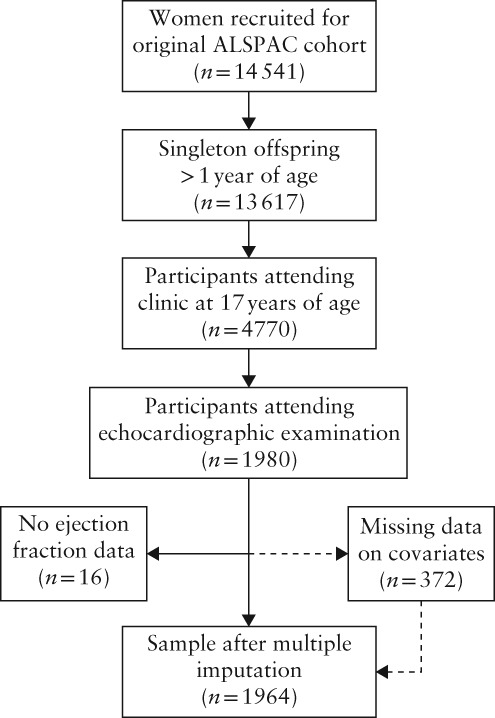
Methods: A subset of offspring (n = 1964; 55% female) of the Avon Longitudinal Study of Parents and Children were examined with echocardiography at a mean age of 17.7 (SD, 0.3) years. The associations of birth-weight Z-score for sex and gestational age with cardiac structure (assessed by relative wall thickness, left ventricular mass index (LVMI) and left atrial diameter index), systolic function (assessed by ejection fraction and left ventricular wall velocity) and diastolic function (assessed by early/late mitral inflow velocity (E/A) and early mitral inflow velocity/mitral annular early diastolic velocity (E/e')) were evaluated. Linear regression models were adjusted for several potential confounders, including maternal prepregnancy body mass index, age, level of education and smoking during pregnancy.
Results: Higher birth-weight Z-score was associated with lower E/A (mean difference, -0.024; 95% CI, -0.043 to -0.005) and E/e' (mean difference, -0.05; 95% CI, -0.10 to -0.001) and higher LVMI (mean difference, 0.38 g/m2.7 ; 95% CI, 0.09 to 0.67). There was no or inconsistent evidence of associations of birth-weight Z-score with relative wall thickness, left atrial diameter and measurements of systolic function. Further analyses suggested that the association between birth-weight Z-score and LVMI was driven mainly by an association observed in participants born small-for-gestational age and it did not persist when risk factors in adolescence were accounted for.
Conclusions: Higher birth weight adjusted for sex and gestational age was associated with differences in measures of diastolic function in adolescence, but the observed associations were small. It remains to be determined the extent to which these associations translate into increased susceptibility to cardiovascular disease later in life. © 2018 The Authors. Ultrasound in Obstetrics & Gynecology published by John Wiley & Sons Ltd on behalf of the International Society of Ultrasound in Obstetrics and Gynecology.
Keywords: ALSPAC; cardiac development; echocardiography; epidemiology; fetal growth restriction.
© 2018 The Authors. Ultrasound in Obstetrics & Gynecology published by John Wiley & Sons Ltd on behalf of the International Society of Ultrasound in Obstetrics and Gynecology.
Figures
References
-
- Barker DJP, Osmond C, Winter PD, Margetts B, Simmonds SJ. Weight in infancy and death from ischemic heart disease. Lancet 1989; 334: 577–580. - PubMed
-
- Lynch J, Smith GD. A Life Course Approach to Chronic Disease Epidemiology. Annu Rev Public Health 2005; 26: 1–35. - PubMed
-
- Miller J, Turan S, Baschat AA. Fetal Growth Restriction. Semin Perinatol 2008; 32: 274–280. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
