

Variation in Case-Mix Adjusted Unplanned Pediatric Cardiac ICU Readmission Rates
- PMID: 30252712
- PMCID: PMC6239958
- DOI: 10.1097/CCM.0000000000003440
Variation in Case-Mix Adjusted Unplanned Pediatric Cardiac ICU Readmission Rates
Abstract
Objectives: To identify modifiable factors leading to unplanned readmission and characterize differences in adjusted unplanned readmission rates across hospitals.
Design: Retrospective cohort study using prospectively collected clinical registry data SETTING:: Pediatric Cardiac Critical Care Consortium clinical registry.
Patients: Patients admitted to a pediatric cardiac ICU at Pediatric Cardiac Critical Care Consortium hospitals.
Interventions: None.
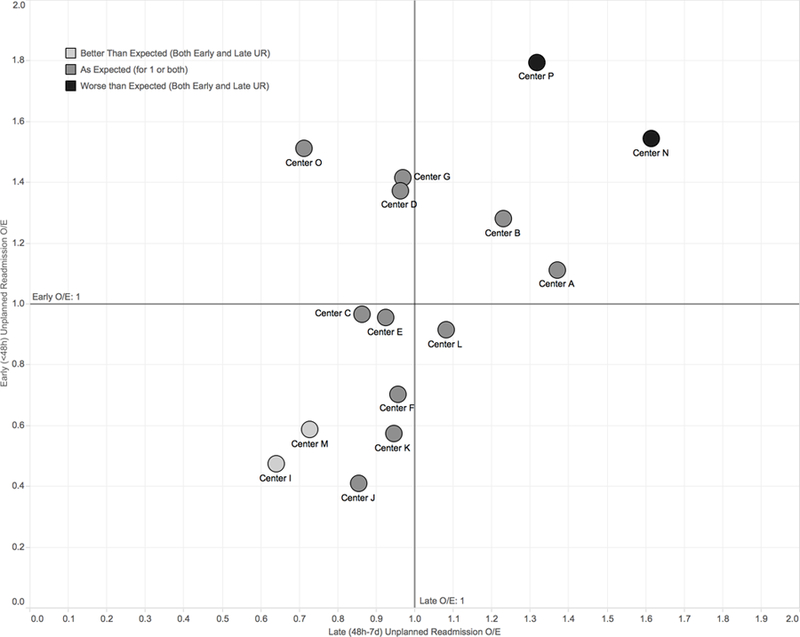
Measurements and main results: We examined pediatric cardiac ICU encounters in the Pediatric Cardiac Critical Care Consortium registry from October 2013 to March 2016. The primary outcomes were early (< 48 hr from pediatric cardiac ICU transfer) and late (2-7 d) unplanned readmission. Generalized logit models identified independent predictors of unplanned readmission. We then calculated observed-to-expected ratios of unplanned readmission and identified higher-than or lower-than-expected unplanned readmission rates for those with an observed-to-expected ratios greater than or less than 1, respectively, and a 95% CI that did not cross 1. Of 11,301 pediatric cardiac ICU encounters (16 hospitals), 62% were surgical, and 18% were neonates. There were 175 (1.6%) early unplanned readmission, and 300 (2.7%) late unplanned readmission, most commonly for respiratory (31%), or cardiac (28%) indications. In multivariable analysis, unique modifiable factors were associated with unplanned readmission. Although shorter time between discontinuation of vasoactive infusions and pediatric cardiac ICU transfer was associated with early unplanned readmission, nighttime discharge was independently associated with a greater likelihood of late unplanned readmission. Two hospitals had lower-than-expected unplanned readmission in both the early and late categories, whereas two other hospitals were higher-than-expected in both.
Conclusions: This analysis demonstrated time from discontinuation of critical care therapies to pediatric cardiac ICU transfer as a significant, modifiable predictor of unplanned readmission. We identified two hospitals with lower-than-expected adjusted rates of both early and late unplanned readmission, suggesting that their systems are well designed to prevent unplanned readmission. This offers the possibility of disseminating best practices to other hospitals through collaborative learning.
Conflict of interest statement
The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Comment in
-
ICU Readmission Is a More Complex Metric Than We First Imagined.Crit Care Med. 2018 Dec;46(12):2064-2067. doi: 10.1097/CCM.0000000000003480. Crit Care Med. 2018. PMID: 30444819 No abstract available.
-
Assumption Versus Knowledge.Crit Care Med. 2019 Mar;47(3):e267-e268. doi: 10.1097/CCM.0000000000003539. Crit Care Med. 2019. PMID: 30768517 No abstract available.
-
The authors reply.Crit Care Med. 2019 Mar;47(3):e268-e269. doi: 10.1097/CCM.0000000000003588. Crit Care Med. 2019. PMID: 30768518 No abstract available.
References
-
- Rosenberg AL, Watts C: Patients readmitted to ICUs* : a systematic review of risk factors and outcomes. Chest 2000; 118:492–502 - PubMed
-
- Rosenberg AL, Hofer TP, Hayward RA, et al. : Who bounces back? Physiologic and other predictors of intensive care unit readmission. Crit Care Med 2001; 29:511–8 - PubMed
-
- Kramer AA, Higgins TL, Zimmerman JE: Intensive care unit readmissions in U.S. hospitals: patient characteristics, risk factors, and outcomes. Crit Care Med 2012; 40:3–10 - PubMed
-
- Renton J, Pilcher DV, Santamaria JD, et al. : Factors associated with increased risk of readmission to intensive care in Australia. Intensive Care Med 2011; 37:1800–1808 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
