

Variations in the quality of tuberculosis care in urban India: A cross-sectional, standardized patient study in two cities
- PMID: 30252849
- PMCID: PMC6155454
- DOI: 10.1371/journal.pmed.1002653
Variations in the quality of tuberculosis care in urban India: A cross-sectional, standardized patient study in two cities
Abstract
Background: India has the highest burden of tuberculosis (TB). Although most patients with TB in India seek care from the private sector, there is limited evidence on quality of TB care or its correlates. Following our validation study on the standardized patient (SP) method for TB, we utilized SPs to examine quality of adult TB care among health providers with different qualifications in 2 Indian cities.
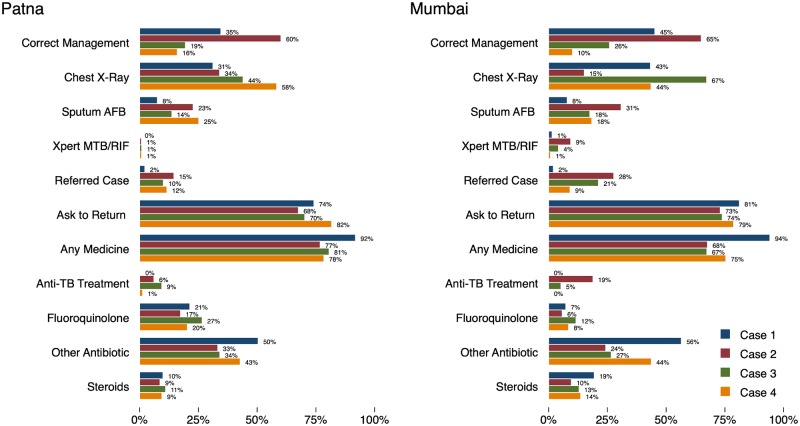
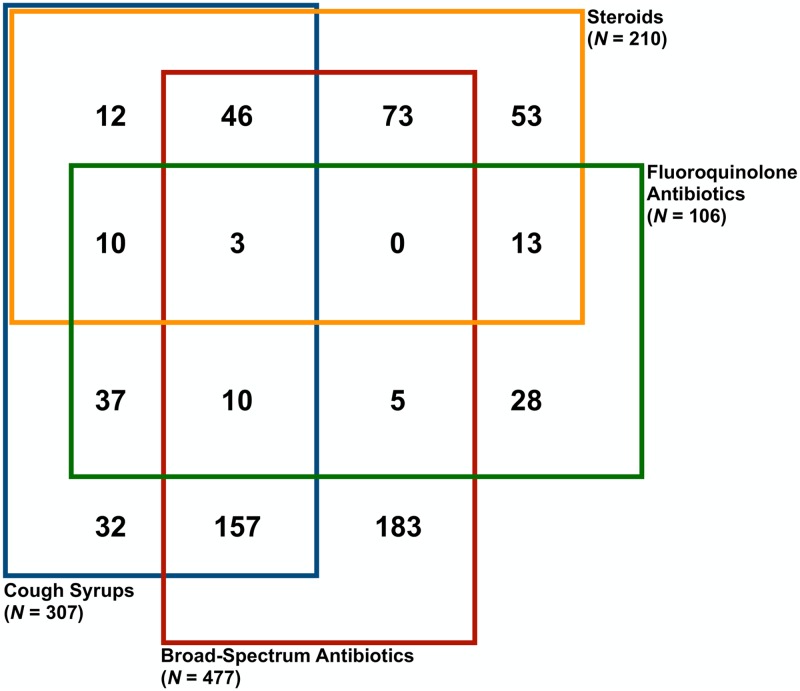
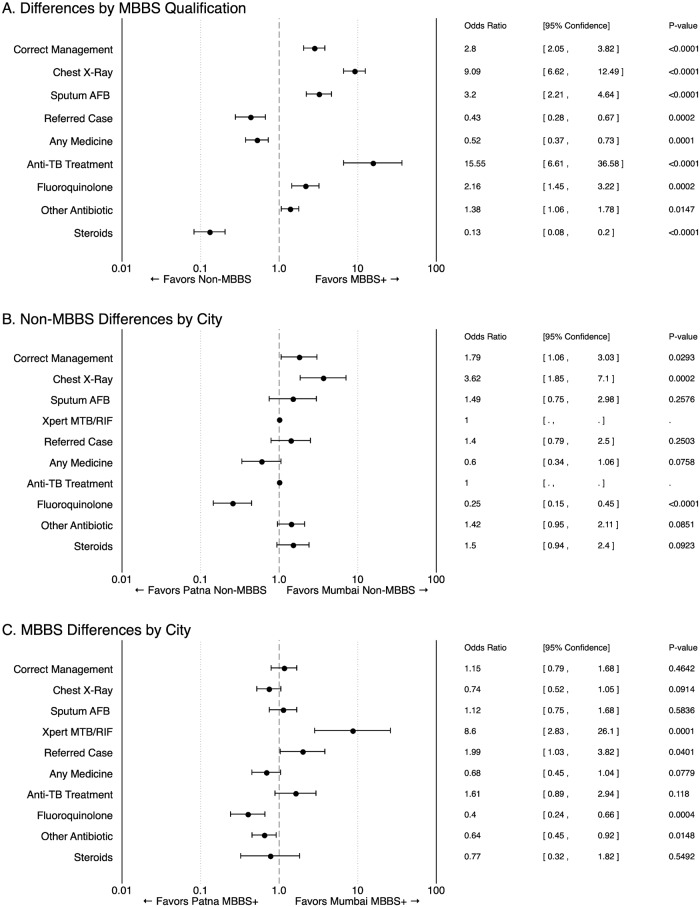
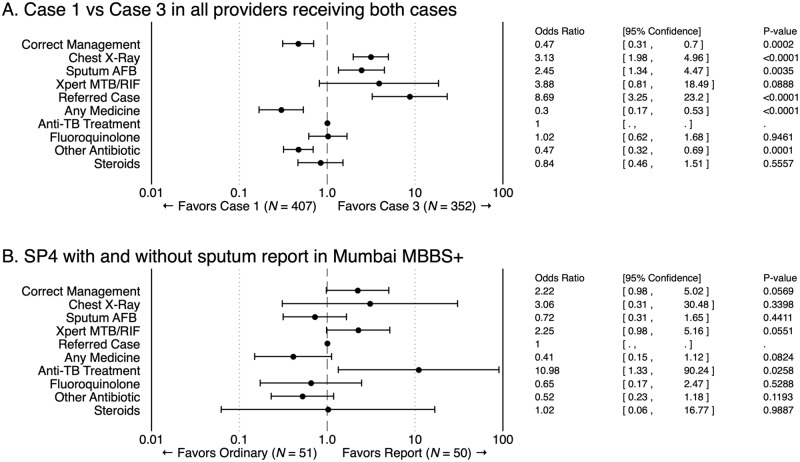
Methods and findings: During 2014-2017, pilot programs engaged the private health sector to improve TB management in Mumbai and Patna. Nested within these projects, to obtain representative, baseline measures of quality of TB care at the city level, we recruited 24 adults to be SPs. They were trained to portray 4 TB "case scenarios" representing various stages of disease and diagnostic progression. Between November 2014 and August 2015, the SPs visited representatively sampled private providers stratified by qualification: (1) allopathic providers with Bachelor of Medicine, Bachelor of Surgery (MBBS) degrees or higher and (2) non-MBBS providers with alternative medicine, minimal, or no qualifications. Our main outcome was case-specific correct management benchmarked against the Standards for TB Care in India (STCI). Using ANOVA, we assessed variation in correct management and quality outcomes across (a) cities, (b) qualifications, and (c) case scenarios. Additionally, 2 micro-experiments identified sources of variation: first, quality in the presence of diagnostic test results certainty and second, provider consistency for different patients presenting the same case. A total of 2,652 SP-provider interactions across 1,203 health facilities were analyzed. Based on our sampling strategy and after removing 50 micro-experiment interactions, 2,602 interactions were weighted for city-representative interpretation. After weighting, the 473 Patna providers receiving SPs represent 3,179 eligible providers in Patna; in Mumbai, the 730 providers represent 7,115 eligible providers. Correct management was observed in 959 out of 2,602 interactions (37%; 35% weighted; 95% CI 32%-37%), primarily from referrals and ordering chest X-rays (CXRs). Unnecessary medicines were given to nearly all SPs, and antibiotic use was common. Anti-TB drugs were prescribed in 118 interactions (4.5%; 5% weighted), of which 45 were given in the case in which such treatment is considered correct management. MBBS and more qualified providers had higher odds of correctly managing cases than non-MBBS providers (odds ratio [OR] 2.80; 95% CI 2.05-3.82; p < 0.0001). Mumbai non-MBBS providers had higher odds of correct management than non-MBBS in Patna (OR 1.79; 95% CI 1.06-3.03), and MBBS providers' quality of care did not vary between cities (OR 1.15; 95% CI 0.79-1.68; p = 0.4642). In the micro-experiments, improving diagnostic certainty had a positive effect on correct management but not across all quality dimensions. Also, providers delivered idiosyncratically consistent care, repeating all observed actions, including mistakes, approximately 75% of the time. The SP method has limitations: it cannot account for patient mix or care-management practices reflecting more than one patient-provider interaction.
Conclusions: Quality of TB care is suboptimal and variable in urban India's private health sector. Addressing this is critical for India's plans to end TB by 2025. For the first time, we have rich measures on representative levels of care quality from 2 cities, which can inform private-sector TB interventions and quality-improvement efforts.
Conflict of interest statement
We have read the journal’s policy, and the authors of this manuscript have the following competing interests: MP is a member of the Editorial Boards of PLOS Medicine and PLOS ONE and is also an editor of the PLOS Tuberculosis Channel. MP previously served as a consultant to the Bill & Melinda Gates Foundation. The other authors have no competing interests to declare.
Figures
Similar articles
-
Predicting the impact of patient and private provider behavior on diagnostic delay for pulmonary tuberculosis patients in India: A simulation modeling study.PLoS Med. 2020 May 14;17(5):e1003039. doi: 10.1371/journal.pmed.1003039. eCollection 2020 May. PLoS Med. 2020. PMID: 32407407 Free PMC article.
-
Use of standardised patients to assess quality of tuberculosis care: a pilot, cross-sectional study.Lancet Infect Dis. 2015 Nov;15(11):1305-13. doi: 10.1016/S1473-3099(15)00077-8. Epub 2015 Aug 9. Lancet Infect Dis. 2015. PMID: 26268690 Free PMC article.
-
Use of standardised patients to assess gender differences in quality of tuberculosis care in urban India: a two-city, cross-sectional study.Lancet Glob Health. 2019 May;7(5):e633-e643. doi: 10.1016/S2214-109X(19)30031-2. Epub 2019 Mar 27. Lancet Glob Health. 2019. PMID: 30928341 Free PMC article.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Knowledge, attitudes and practices of private sector providers of tuberculosis care: a scoping review.Int J Tuberc Lung Dis. 2011 Aug;15(8):1005-17. doi: 10.5588/ijtld.10.0294. Int J Tuberc Lung Dis. 2011. PMID: 21669027
Cited by
-
Assessing Medical Emergency E-referral Request Acceptance Patterns and Trends: A Comprehensive Analysis of Secondary Data From the Kingdom of Saudi Arabia.Cureus. 2024 Feb 3;16(2):e53511. doi: 10.7759/cureus.53511. eCollection 2024 Feb. Cureus. 2024. PMID: 38314384 Free PMC article.
-
User-experience and patient satisfaction with quality of tuberculosis care in India: A mixed-methods literature review.J Clin Tuberc Other Mycobact Dis. 2019 Oct 25;17:100127. doi: 10.1016/j.jctube.2019.100127. eCollection 2019 Dec. J Clin Tuberc Other Mycobact Dis. 2019. PMID: 31788569 Free PMC article. Review.
-
Barriers to engagement in the care cascade for tuberculosis disease in India: A systematic review of quantitative studies.PLoS Med. 2024 May 28;21(5):e1004409. doi: 10.1371/journal.pmed.1004409. eCollection 2024 May. PLoS Med. 2024. PMID: 38805509 Free PMC article.
-
Using unannounced standardised patients to obtain data on quality of care in low-income and middle-income countries: key challenges and opportunities.BMJ Glob Health. 2019 Sep 12;4(5):e001908. doi: 10.1136/bmjgh-2019-001908. eCollection 2019. BMJ Glob Health. 2019. PMID: 31565422 Free PMC article. No abstract available.
-
Know-do gaps for cardiovascular disease care in Cambodia: Evidence on clinician knowledge and delivery of evidence-based prevention actions.PLOS Glob Public Health. 2022 Sep 1;2(9):e0000862. doi: 10.1371/journal.pgph.0000862. eCollection 2022. PLOS Glob Public Health. 2022. PMID: 36962790 Free PMC article.
References
-
- World Health Organization. Global Tuberculosis Report 2017. Geneva: WHO; 2017.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
