

Comparative effectiveness of radical prostatectomy with adjuvant radiotherapy versus radiotherapy plus androgen deprivation therapy for men with advanced prostate cancer
- PMID: 30252932
- PMCID: PMC6234085
- DOI: 10.1002/cncr.31726
Comparative effectiveness of radical prostatectomy with adjuvant radiotherapy versus radiotherapy plus androgen deprivation therapy for men with advanced prostate cancer
Abstract
Background: Men with locally advanced prostate cancer (LAPCa) or regionally advanced prostate cancer (RAPCa) are at high risk for death from their disease. Clinical guidelines support multimodal approaches, which include radical prostatectomy (RP) followed by radiotherapy (XRT) and XRT plus androgen deprivation therapy (ADT). However, there are limited data comparing these substantially different treatment approaches. Using Surveillance, Epidemiology, and End Results (SEER)-Medicare data, this study compared survival outcomes and adverse effects associated with RP plus XRT versus XRT plus ADT in these men.
Methods: SEER-Medicare data were queried for men with cT3-T4N0M0 (LAPCa) or cT3-T4N1M0 (RAPCa) prostate cancer. Propensity score methods were used to balance cohort characteristics between the treatment arms. Survival analyses were analyzed with the Kaplan-Meier method and Cox proportional hazards models.
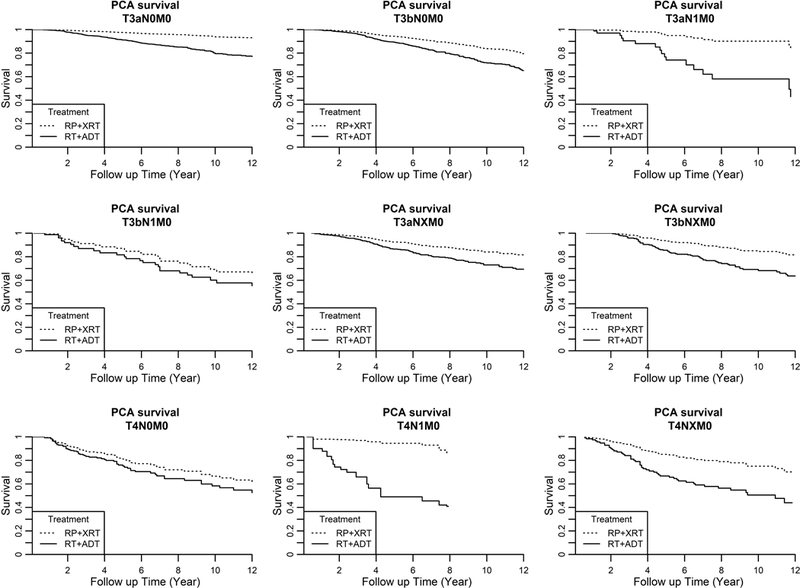
Results: From 1992 to 2009, 13,856 men (≥65 years old) were diagnosed with LAPCa or RAPCa: 6.1% received RP plus XRT, and 23.6% received XRT plus ADT. At a median follow-up of 14.6 years, there were 2189 deaths in the cohort, of which 702 were secondary to prostate cancer. Regardless of the tumor stage or the Gleason score, the adjusted 10-year prostate cancer-specific survival and 10-year overall survival favored men who underwent RP plus XRT over men who underwent XRT plus ADT. However, RP plus XRT versus XRT plus ADT was associated with higher rates of erectile dysfunction (28% vs 20%; P = .0212) and urinary incontinence (49% vs 19%; P < .001).
Conclusions: Men with LAPCa or RAPCa treated initially with RP plus XRT had a lower risk of prostate cancer-specific death and improved overall survival in comparison with those men treated with XRT plus ADT, but they experienced higher rates of erectile dysfunction and urinary incontinence.
Keywords: combined modality therapy; comparative effectiveness; hormone therapy; outcomes; population and observational studies; prostate cancer; radiation; surgery; survival.
© 2018 American Cancer Society.
Conflict of interest statement
Conflict of Interest Disclosures:
Dr. Jang reports grants from National Cancer Institute (P30 CA-072720), grants from New Jersey Health Foundation, during the conduct of the study.
Dr. Scardino reports other from OPKO, outside the submitted work (Clinical Advisory Board); In addition, Dr. Scardino has a patent OPKO issued.
Dr. Stein reports personal fees from Merck, outside the submitted work;
All other authors declare no competing interests.
Figures

Comment in
-
Effectiveness of radical prostatectomy with adjuvant radiotherapy versus radiotherapy plus androgen deprivation therapy for men with advanced prostate cancer: Do we have certainties today?Cancer. 2019 Jul 1;125(13):2318. doi: 10.1002/cncr.32055. Epub 2019 Mar 12. Cancer. 2019. PMID: 30861092 No abstract available.
-
Reply to Effectiveness of radical prostatectomy with adjuvant radiotherapy versus radiotherapy plus androgen deprivation therapy for men with advanced prostate cancer: Do we have certainties today?Cancer. 2019 Jul 1;125(13):2318-2320. doi: 10.1002/cncr.32054. Epub 2019 Mar 12. Cancer. 2019. PMID: 30861093 No abstract available.
Similar articles
-
Survival and secondary interventions following treatment for locally-advanced prostate cancer.Can J Urol. 2018 Oct;25(5):9516-9524. Can J Urol. 2018. PMID: 30281010
-
Effectiveness of androgen-deprivation therapy and radiotherapy for older men with locally advanced prostate cancer.J Clin Oncol. 2015 Mar 1;33(7):716-22. doi: 10.1200/JCO.2014.57.2743. Epub 2015 Jan 5. J Clin Oncol. 2015. PMID: 25559808 Free PMC article.
-
Improved Survival With Prostate Radiation in Addition to Androgen Deprivation Therapy for Men With Newly Diagnosed Metastatic Prostate Cancer.J Clin Oncol. 2016 Aug 20;34(24):2835-42. doi: 10.1200/JCO.2016.67.4788. Epub 2016 Jun 20. J Clin Oncol. 2016. PMID: 27325855
-
Comparison of Radical Prostatectomy Versus Radiation and Androgen Deprivation Therapy Strategies as Primary Treatment for High-risk Localized Prostate Cancer: A Systematic Review and Meta-analysis.Eur Urol Focus. 2020 Mar 15;6(2):404-418. doi: 10.1016/j.euf.2019.11.007. Epub 2019 Dec 5. Eur Urol Focus. 2020. PMID: 31813810
-
Abiraterone acetate in combination with androgen deprivation therapy compared to androgen deprivation therapy only for metastatic hormone-sensitive prostate cancer.Cochrane Database Syst Rev. 2020 Dec 12;12(12):CD013245. doi: 10.1002/14651858.CD013245.pub2. Cochrane Database Syst Rev. 2020. PMID: 33314020 Free PMC article.
Cited by
-
Supported progressive resistance exercise training to counter the adverse side effects of robot-assisted radical prostatectomy: a randomised controlled trial.Support Care Cancer. 2021 Aug;29(8):4595-4605. doi: 10.1007/s00520-021-06002-5. Epub 2021 Jan 23. Support Care Cancer. 2021. PMID: 33483790 Free PMC article. Clinical Trial.
-
Multimodal treatments for advanced prostate cancer.Oncotarget. 2019 Jan 8;10(3):255-256. doi: 10.18632/oncotarget.26525. eCollection 2019 Jan 8. Oncotarget. 2019. PMID: 30719221 Free PMC article. No abstract available.
-
Dose-escalated pelvic radiotherapy for prostate cancer in definitive or postoperative setting.Radiol Med. 2022 Feb;127(2):206-213. doi: 10.1007/s11547-021-01435-8. Epub 2021 Nov 30. Radiol Med. 2022. PMID: 34850352
-
Geriatric conditions and treatment burden following diagnosis of non-muscle- invasive bladder cancer in older adults: A population-based analysis.J Geriatr Oncol. 2021 Sep;12(7):1022-1030. doi: 10.1016/j.jgo.2021.04.005. Epub 2021 May 8. J Geriatr Oncol. 2021. PMID: 33972184 Free PMC article.
-
Comparative Survival Outcomes of High-risk Prostate Cancer Treated with Radical Prostatectomy or Definitive Radiotherapy Regimens.Eur Urol Open Sci. 2021 Feb 24;26:55-63. doi: 10.1016/j.euros.2021.01.011. eCollection 2021 Apr. Eur Urol Open Sci. 2021. PMID: 34337508 Free PMC article.
References
-
- Siegel RL, Miller KD, Jemal A. Cancer Statistics, 2017. CA Cancer J Clin 2017;67: 7–30. - PubMed
-
- Mottet N, Bellmunt J, Bolla M, et al. EAU-ESTRO-SIOG Guidelines on Prostate Cancer. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur Urol 2017;71: 618–629. - PubMed
-
- Mohler JL, Armstrong AJ, Bahnson RR, et al. Prostate Cancer, Version 1.2016. J Natl Compr Canc Netw 2016;14: 19–30. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
