

Likelihood of cesarean birth among parous women after applying leading active labor diagnostic guidelines
- PMID: 30253316
- PMCID: PMC6217861
- DOI: 10.1016/j.midw.2018.09.007
Likelihood of cesarean birth among parous women after applying leading active labor diagnostic guidelines
Abstract
Objectives: Hospital admission during early labor may increase women's risk for medical and surgical interventions. However, it is unclear which diagnostic guideline is best suited for identifying the active phase of labor among parous women. Dr. Emanuel Friedman, the United Kingdom's National Institute for Health and Care Excellence (NICE), and the American College of Obstetricians and Gynecologists/Society for Maternal-Fetal Medicine (ACOG/SMFM) support different active labor diagnostic guidelines. Our aims were (1) to determine the proportions of parous women admitted to the hospital before or in active labor per these leading guidelines and (2) to compare associations of labor status at admission (i.e., early labor or active labor) with oxytocin augmentation, cesarean birth, and adverse birth outcomes when using the different active labor diagnostic guidelines.
Design: Active labor diagnostic guidelines were applied retrospectively to cervical examination data. Binomial logistic regression was used to assess associations of labor status at admission (i.e., early labor relative to active labor) and outcomes.
Setting: A large, academic, tertiary medical center in the Midwestern United States.
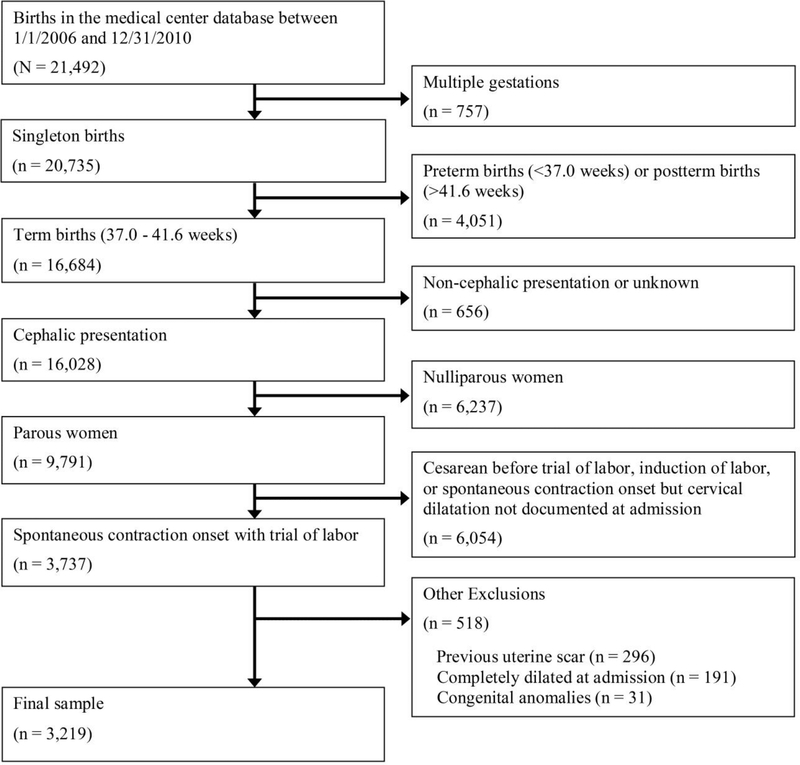
Participants: Parous women with spontaneous labor onset who gave birth to a single, cephalic-presenting fetus at term gestation between 2006 and 2010 (n = 3,219).
Findings: At admission, 28.8%, 71.9%, and 24.4% of parous women were in active labor per Friedman, NICE, and ACOG/SMFM diagnostic guidelines, respectively. Oxytocin augmentation was more likely among women admitted in early labor, regardless of the diagnostic strategy used (p < 0.001 for each guideline). Cesarean birth was also more likely among women admitted before versus in active labor according to all guidelines (Friedman: adjusted odds ratio [AOR] 3.63 [95% CI 1.46-9.03]), NICE: AOR 2.71 [95% CI 1.47-4.99]), and ACOG/SMFM: AOR 2.11 [95% CI 1.02-4.34]). There were no differences in a composite measure of adverse outcomes within active labor diagnostic guidelines after adjusting for covariates.
Key conclusions: Many parous women with spontaneous labor onset are admitted to the hospital before active labor. These women are more likely to receive oxytocin augmentation during labor and are more likely to have a cesarean birth.
Implications for practice: Diagnosing active labor prior to admission or prior to intervention aimed at speeding labor after admission may decrease likelihoods for primary cesarean births. The NICE dilation-rate based active labor diagnostic guideline is more inclusive than Friedman or ACOG/SMFM guidelines and its use may be the most clinically-useful for improving the likelihood of vaginal birth among parous women.
Keywords: Cesarean section; Labor onset; Labor stage, First; Oxytocin; Parity; Parturition.
Copyright © 2018 Elsevier Ltd. All rights reserved.
References
-
- American College of Obstetricians and Gynecologists, 2017. Committee Opinion No. 687: Approaches to limit intervention during labor and birth. Obstetrics and gynecology 129, e20–8. - PubMed
-
- Bailit JL, Dierker L, Blanchard MH, Mercer BM, 2005. Outcomes of women presenting in active versus latent phase of spontaneous labor. Obstetrics and gynecology 105, 77–9. - PubMed
-
- Bovbjerg ML, Cheyney M, Brown J, Cox KJ, Leeman L, 2017. Perspectives on risk: Assessment of risk profiles and outcomes among women planning community birth in the United States. Birth (Berkeley, Calif.) 44, 209–21. - PubMed
-
- Caughey AB, Cahill AG, Guise J, Rouse DJ, 2014. Safe prevention of the primary cesarean delivery. American Journal of Obstetrics and Gynecology 210, 179–93. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
