

Endoscopic Ultrasound with Bronchoscope-Guided Fine Needle Aspiration for the Diagnosis of Paraesophageally Located Lung Lesions
- PMID: 30253411
- PMCID: PMC6518855
- DOI: 10.1159/000492578
Endoscopic Ultrasound with Bronchoscope-Guided Fine Needle Aspiration for the Diagnosis of Paraesophageally Located Lung Lesions
Abstract
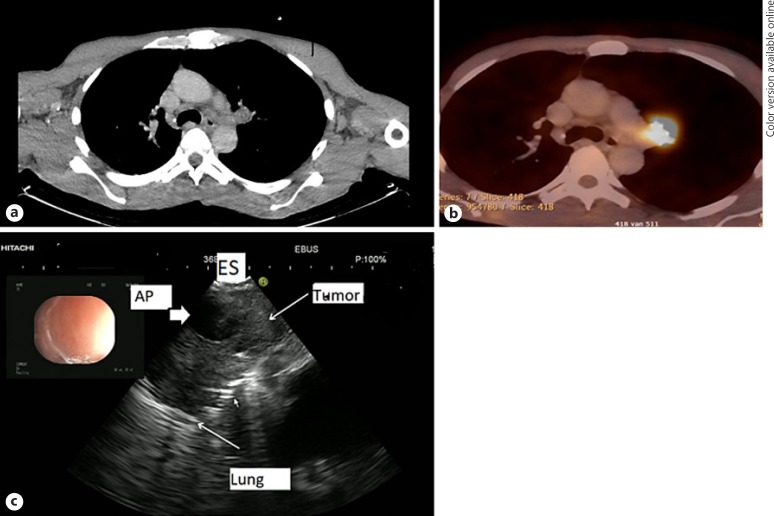
Background: Diagnosing centrally located lung tumors without endobronchial abnormalities and not located near the major airways is a diagnostic challenge. Tumors near or adjacent to the esophagus can be aspirated and detected with esophageal ultrasound (EUS) using gastrointestinal endoscopes.
Objective: To assess the feasibility and diagnostic yield of endoscopic ultrasound with bronchoscope-guided fine needle aspiration (EUS-B-FNA) in paraesophageally located lung tumors and its added value to bronchoscopy and endobronchial ultrasound (EBUS).
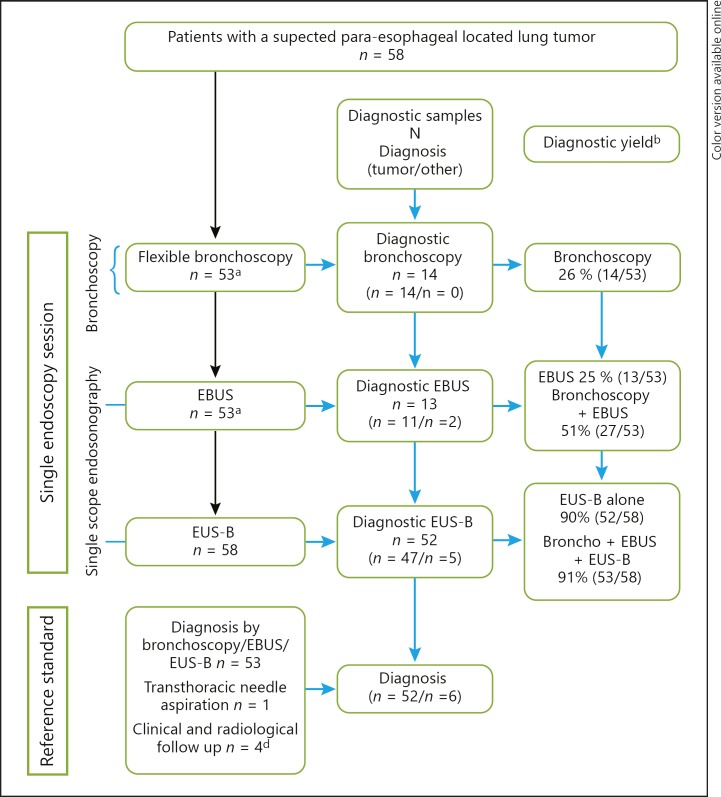
Methods: Retrospective, multicenter international study (from January 1, 2015 until January 1, 2018) of patients with suspected lung cancer, undergoing bronchoscopy, EBUS, and endoscopic ultrasound bronchoscopy (EUS-B) in one session by a single operator (pulmonologist), in whom the primary lung tumor was detected and aspirated by EUS-B. In the absence of malignancy following endoscopy, transthoracic ultrasound needle aspiration, clinical and radiological follow-up of at least 6 months was performed. The yield and sensitivity of EUS-B-FNA and its added value to bronchoscopy and EBUS was assessed.
Results: 58 patients were identified with the following diagnosis: non-small-cell lung cancer (n = 43), small-cell lung cancer (n = 6), mesothelioma (n = 2), metastasis (n = 1), nonmalignant (n = 6). The yield and sensitivity of EUS-B-FNA for detecting lung cancer was 90%. In 26 patients (45%), the intrapulmonary tumor was exclusively detected by EUS-B. Adding EUS-B to conventional bronchoscopy and EBUS increased the diagnostic yield for diagnosing lung cancer in para-esophageally located lung tumors from 51 to 91%. No EUS-B-related complications were observed.
Conclusion: EUS-B-FNA is a feasible and safe technique for diagnosing centrally located intrapulmonary tumors that are located near or adjacent to the esophagus. EUS-B should be considered in the same endoscopy session following nondiagnostic bronchoscopy and EBUS.
Keywords: Diagnosis; Endobronchial ultrasound; Esophageal ultrasound; Lung cancer.
© 2018 The Author(s) Published by S. Karger AG, Basel.
Figures
References
-
- Global Burden. of Disease Cancer Collaboration Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 32 cancer groups, 1990 to 2015: a systematic analysis for the global burden of disease study. JAMA Oncol. 2017;3:524–548. - PMC - PubMed
-
- Rivera MP, Mehta AC, Wahidi MM. Establishing the diagnosis of lung cancer: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013;143((5 Suppl)):e142S–e165S. - PubMed
-
- Du Rand IA, Barber PV, Goldring J, Lewis RA, Mandal S, Munavvar M, et al. British Thoracic Society guideline for advanced diagnostic and therapeutic flexible bronchoscopy in adults. Thorax. 2011;66:iii1–iii21. - PubMed
-
- Popovich J, Kvale PA, Eichenhorn MS, Radke , Jr, Ohorodnik JM, Fine G. Diagnostic accuracy of multiple biopsies from flexible fiberoptic bronchoscopy. Am Rev Respir Dis. 1982;125:521–523. - PubMed
-
- Mazzone P, Jain P, Arroliga AC, Matthay RA. Bronchoscopy and needle biopsy techniques for diagnosis and staging of lung cancer. Clin Chest Med. 2002;23:137–158. ix. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
