

Resistant Streptococcus pneumoniae strains in children with acute otitis media- high risk of persistent colonization after treatment
- PMID: 30253754
- PMCID: PMC6156860
- DOI: 10.1186/s12879-018-3398-9
Resistant Streptococcus pneumoniae strains in children with acute otitis media- high risk of persistent colonization after treatment
Abstract
Background: Despite advances in the development of pneumococcal conjugate vaccines, acute otitis media (AOM) is a common childhood infection, caused mainly by Streptococcus pneumoniae. It has been suggested that persistence of pneumococcal nasopharyngeal carriage is a risk factor for subsequent recurrent infections.
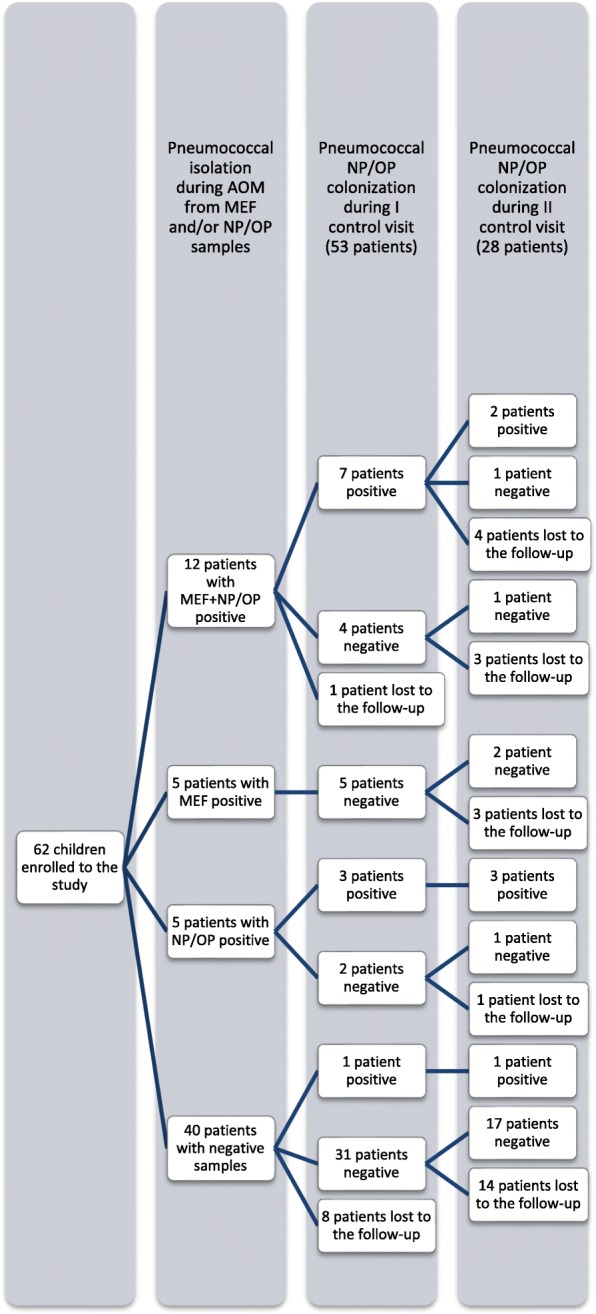
Methods: In this study we evaluate the relationship between 55 pneumococcal strains obtained from nasopharynx/oropharynx (NP/OP) and middle ear fluid (MEF) of 62 children, aged between 1 and 16 years, during AOM (including recurrent/treatment failure AOM, and post-treatment visits), based on their phenotypic and genotypic characteristics performed by analyses of serotype, antibiotic susceptibility patterns and multilocus sequence typing.
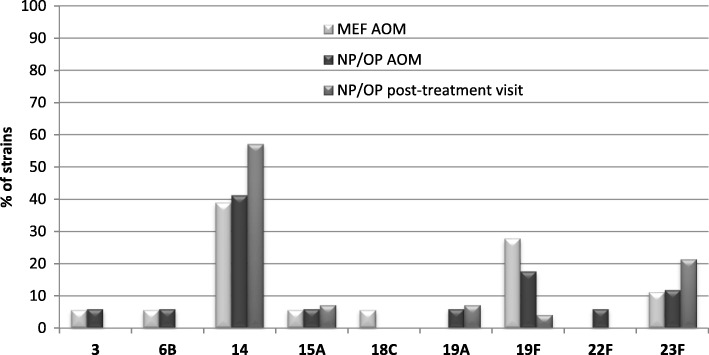
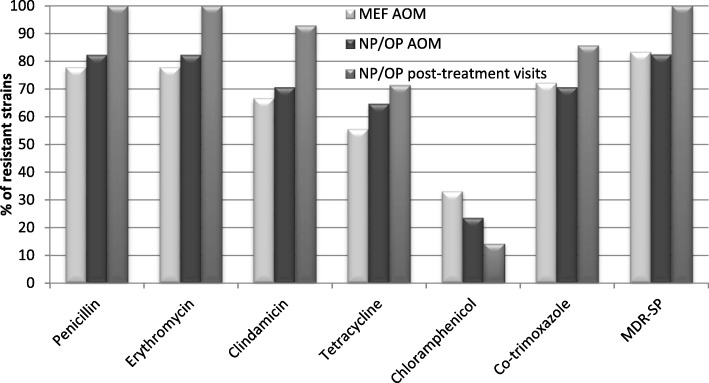
Results: S.pneumoniae was isolated from 27.4% of MEF samples; it constituted 43.6% of all positive bacterial samples from MEF samples. There was statistically significant concordance between isolation from the MEF sample and NP/OP colonization by S. pneumoniae (p < 0.0001). During post-treatment visits S.pneumoniae was isolated from 20.8% of children; 91% of them were positive in pneumococcal NP/OP culture during AOM. The serotypes belonging to 10- and 13-valent pneumococcal conjugated vaccines constituted 84% and 92% of the strains, respectively. Multidrug resistance was found in 84% of the strains. According to multivariate analysis, pneumococcal colonization after antibiotic therapy was significantly associated with shorter length of therapy in children with bilateral AOM.
Conclusions: High persistent prevalence of antibiotic-resistant S.pneumoniae strains in children with AOM after unsuccessful bacterial eradication may presumably be regarded as a predisposing factor of infection recurrence.
Keywords: Acute otitis media; Antibiotic resistance; MLST; Risk factors; Streptococcus pneumoniae.
Conflict of interest statement
Ethics approval and consent to participate
The Ethical Committee of the Medical University of Lublin approved the study protocol (No. KE-0254/75/211). From all children’s parents written informed consent was obtained.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Geng Q, Zhang T, Ding Y, Tao Y, Lin Y, Wang Y, et al. Molecular characterization and antimicrobial susceptibility of Streptococcus pneumoniae isolated from children hospitalized with respiratory infections in Suzhou, China. PlosOne. 2014;9:e93752. doi: 10.1371/journal.pone.0093752. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
