

Automated microscopy for routine malaria diagnosis: a field comparison on Giemsa-stained blood films in Peru
- PMID: 30253764
- PMCID: PMC6157053
- DOI: 10.1186/s12936-018-2493-0
Automated microscopy for routine malaria diagnosis: a field comparison on Giemsa-stained blood films in Peru
Abstract
Background: Microscopic examination of Giemsa-stained blood films remains a major form of diagnosis in malaria case management, and is a reference standard for research. However, as with other visualization-based diagnoses, accuracy depends on individual technician performance, making standardization difficult and reliability poor. Automated image recognition based on machine-learning, utilizing convolutional neural networks, offers potential to overcome these drawbacks. A prototype digital microscope device employing an algorithm based on machine-learning, the Autoscope, was assessed for its potential in malaria microscopy. Autoscope was tested in the Iquitos region of Peru in 2016 at two peripheral health facilities, with routine microscopy and PCR as reference standards. The main outcome measures include sensitivity and specificity of diagnosis of malaria from Giemsa-stained blood films, using PCR as reference.
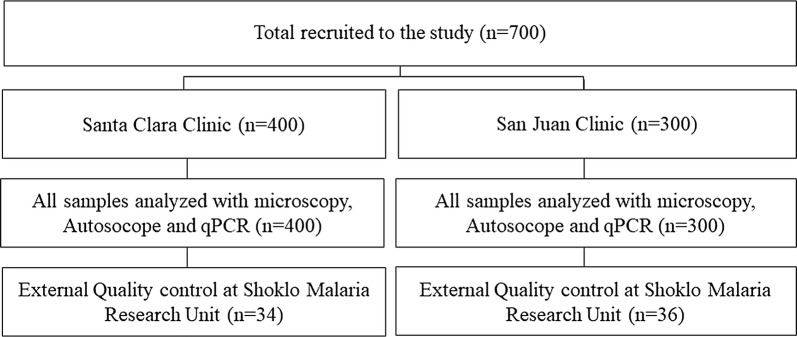
Methods: A cross-sectional, observational trial was conducted at two peripheral primary health facilities in Peru. 700 participants were enrolled with the criteria: (1) age between 5 and 75 years, (2) history of fever in the last 3 days or elevated temperature on admission, (3) informed consent. The main outcome measures included sensitivity and specificity of diagnosis of malaria from Giemsa-stained blood films, using PCR as reference.
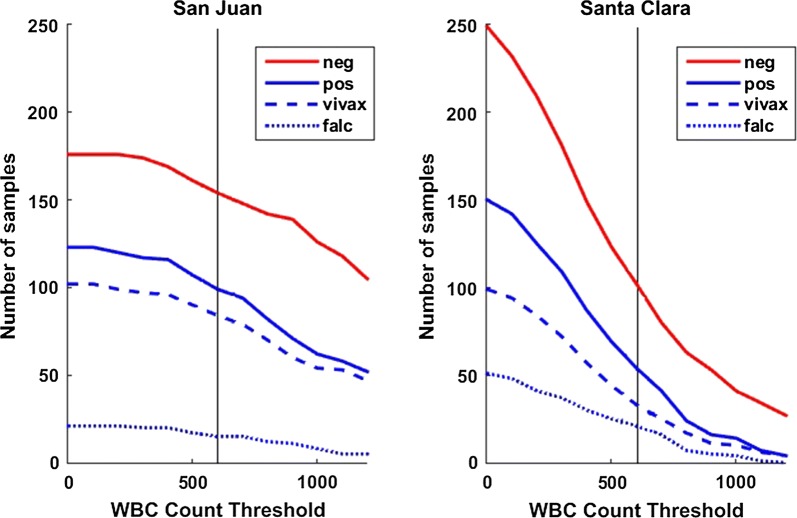
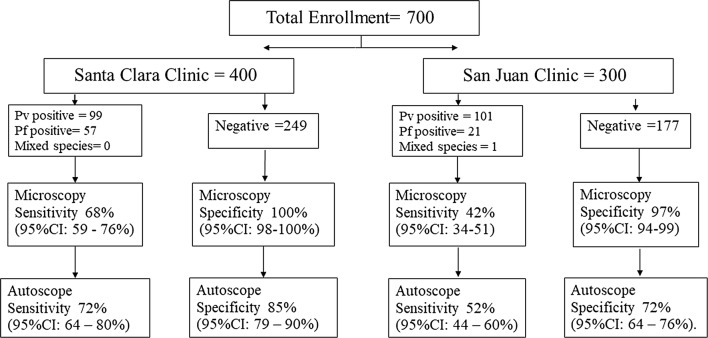
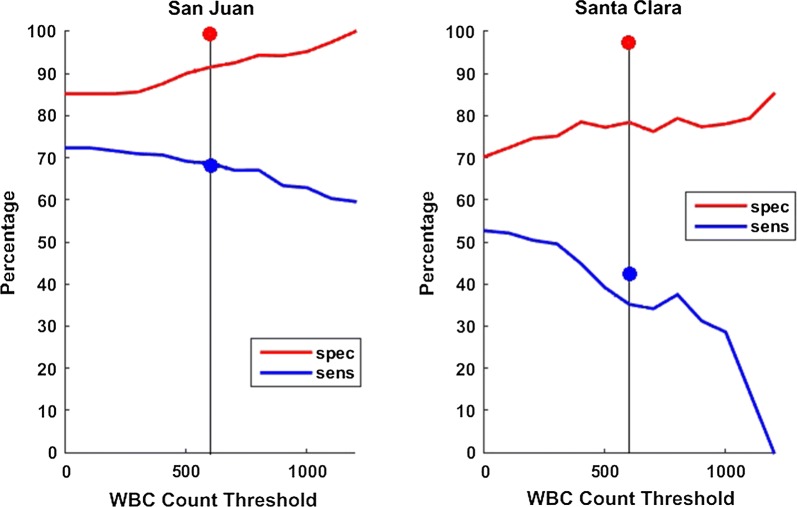
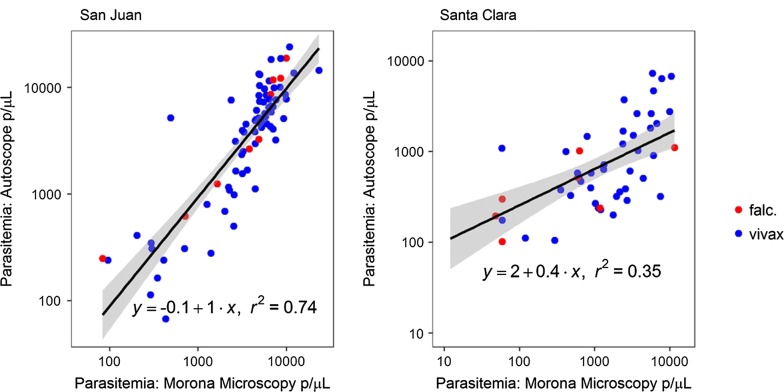
Results: At the San Juan clinic, sensitivity of Autoscope for diagnosing malaria was 72% (95% CI 64-80%), and specificity was 85% (95% CI 79-90%). Microscopy performance was similar to Autoscope, with sensitivity 68% (95% CI 59-76%) and specificity 100% (95% CI 98-100%). At San Juan, 85% of prepared slides had a minimum of 600 WBCs imaged, thus meeting Autoscope's design assumptions. At the second clinic, Santa Clara, the sensitivity of Autoscope was 52% (95% CI 44-60%) and specificity was 70% (95% CI 64-76%). Microscopy performance at Santa Clara was 42% (95% CI 34-51) and specificity was 97% (95% CI 94-99). Only 39% of slides from Santa Clara met Autoscope's design assumptions regarding WBCs imaged.
Conclusions: Autoscope's diagnostic performance was on par with routine microscopy when slides had adequate blood volume to meet its design assumptions, as represented by results from the San Juan clinic. Autoscope's diagnostic performance was poorer than routine microscopy on slides from the Santa Clara clinic, which generated slides with lower blood volumes. Results of the study reflect both the potential for artificial intelligence to perform tasks currently conducted by highly-trained experts, and the challenges of replicating the adaptiveness of human thought processes.
Keywords: Artificial intelligence; Convolutional neural networks; Digital microscopy; Malaria; Microscopy.
Figures
Similar articles
-
Comparison of rapid diagnostic test Plasmotec Malaria-3, microscopy, and quantitative real-time PCR for diagnoses of Plasmodium falciparum and Plasmodium vivax infections in Mimika Regency, Papua, Indonesia.Malar J. 2015 Mar 5;14:103. doi: 10.1186/s12936-015-0615-5. Malar J. 2015. PMID: 25890368 Free PMC article.
-
Field evaluation of the diagnostic performance of EasyScan GO: a digital malaria microscopy device based on machine-learning.Malar J. 2022 Apr 12;21(1):122. doi: 10.1186/s12936-022-04146-1. Malar J. 2022. PMID: 35413904 Free PMC article.
-
Evaluation of the performance of CareStart Malaria Pf/Pv Combo rapid diagnostic test for the diagnosis of malaria in Jimma, southwestern Ethiopia.Acta Trop. 2010 Mar;113(3):285-8. doi: 10.1016/j.actatropica.2009.12.001. Epub 2009 Dec 11. Acta Trop. 2010. PMID: 20005196
-
Assessing field performance of ultrasensitive rapid diagnostic tests for malaria: a systematic review and meta-analysis.Malar J. 2021 Jun 3;20(1):245. doi: 10.1186/s12936-021-03783-2. Malar J. 2021. PMID: 34082776 Free PMC article.
-
Diagnostic tools in childhood malaria.Parasit Vectors. 2018 Jan 23;11(1):53. doi: 10.1186/s13071-018-2617-y. Parasit Vectors. 2018. PMID: 29361963 Free PMC article. Review.
Cited by
-
Plasmodium knowlesi detection methods for human infections-Diagnosis and surveillance.Adv Parasitol. 2021;113:77-130. doi: 10.1016/bs.apar.2021.08.002. Epub 2021 Sep 17. Adv Parasitol. 2021. PMID: 34620386 Free PMC article.
-
Performance of a fully-automated system on a WHO malaria microscopy evaluation slide set.Malar J. 2021 Feb 25;20(1):110. doi: 10.1186/s12936-021-03631-3. Malar J. 2021. PMID: 33632222 Free PMC article.
-
Identification of veterinary and medically important blood parasites using contrastive loss-based self-supervised learning.Vet World. 2024 Nov;17(11):2619-2634. doi: 10.14202/vetworld.2024.2619-2634. Epub 2024 Nov 25. Vet World. 2024. PMID: 39829660 Free PMC article.
-
Automatic patient-level recognition of four Plasmodium species on thin blood smear by a real-time detection transformer (RT-DETR) object detection algorithm: a proof-of-concept and evaluation.Microbiol Spectr. 2024 Feb 6;12(2):e0144023. doi: 10.1128/spectrum.01440-23. Epub 2024 Jan 3. Microbiol Spectr. 2024. PMID: 38171008 Free PMC article.
-
A digital microscope for the diagnosis of Plasmodium falciparum and Plasmodium vivax, including P. falciparum with hrp2/hrp3 deletion.PLOS Glob Public Health. 2024 May 20;4(5):e0003091. doi: 10.1371/journal.pgph.0003091. eCollection 2024. PLOS Glob Public Health. 2024. PMID: 38768243 Free PMC article.
References
-
- Laveran A. Traité des fiévres palustres, avec la description des microbes du paludisme. Paris: Octave Doin; 1884.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
