

Pediatric hepatocellular carcinoma
- PMID: 30254403
- PMCID: PMC6148423
- DOI: 10.3748/wjg.v24.i35.3980
Pediatric hepatocellular carcinoma
Abstract
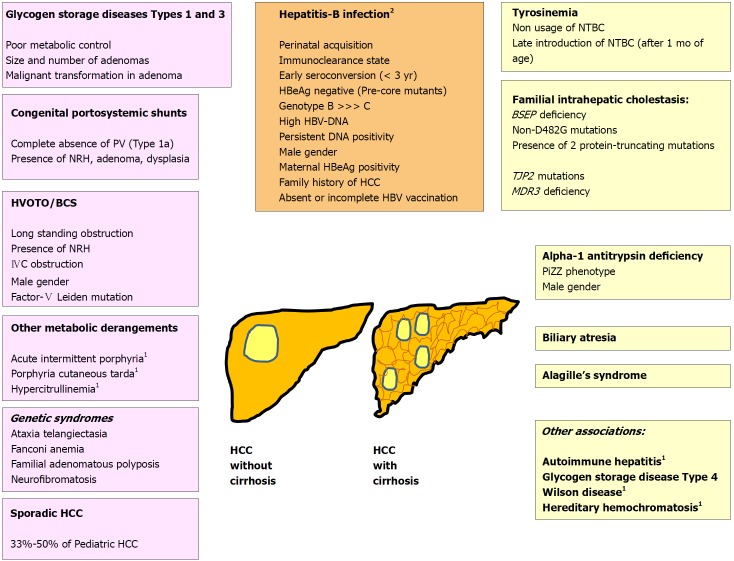
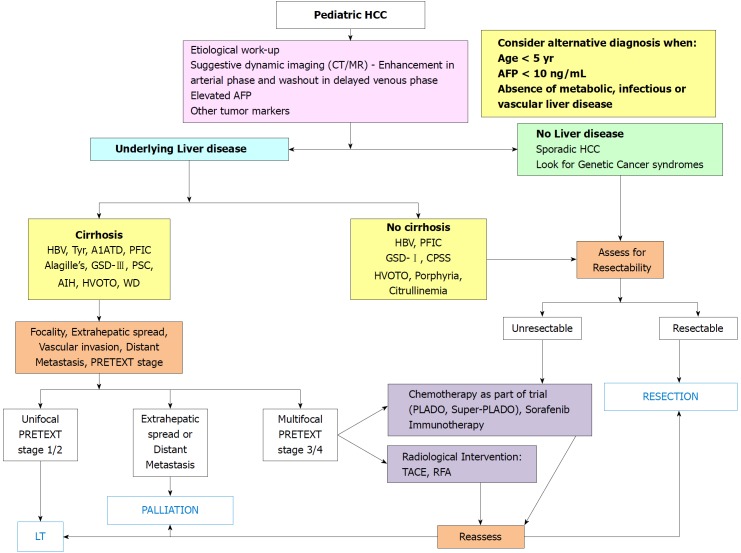
Pediatric hepatocellular carcinoma (HCC) is the second common malignant liver tumor in children after hepatoblastoma. It differs from the adult HCC in the etiological predisposition, biological behavior and lower frequency of cirrhosis. Perinatally acquired hepatitis-B virus, hepatorenal tyrosinemia, progressive familial intrahepatic cholestasis, glycogen storage disease, Alagille's syndrome and congenital portosystemic shunts are important predisposing factors. Majority of children (87%) are older than 5 years of age. Following mass immunization against hepatitis-B, there has been a drastic fall in the incidence of new cases of pediatric HCC in the Asia-Pacific region. Management is targeted on complete surgical removal either by resection or liver transplantation. There is a trend towards improving survival of children transplanted for HCC beyond Milan criteria. Chemotherapeutic regimens do not offer good results but may be helpful for down-staging of advanced HCC. Surveillance of children with chronic liver diseases with ultrasound and alpha-fetoprotein may be helpful in timely detection, intervention and overall improvement in outcome of HCC.
Keywords: Children; Hepatocellular carcinoma; Liver transplantation; Outcome; Risk-factors.
Conflict of interest statement
Conflict-of-interest statement: There are no potential conflicts of interest.
Figures
References
-
- Hadzic N, Finegold MJ. Liver neoplasia in children. Clin Liver Dis. 2011;15:443–462, vii-vix. - PubMed
-
- Kelly D, Sharif K, Brown RM, Morland B. Hepatocellular carcinoma in children. Clin Liver Dis. 2015;19:433–447. - PubMed
-
- Otte JB. Progress in the surgical treatment of malignant liver tumors in children. Cancer Treat Rev. 2010;36:360–371. - PubMed
-
- Ng VL, Fecteau A, Shepherd R, Magee J, Bucuvalas J, Alonso E, McDiarmid S, Cohen G, Anand R; Studies of Pediatric Liver Transplantation Research Group. Outcomes of 5-year survivors of pediatric liver transplantation: report on 461 children from a north american multicenter registry. Pediatrics. 2008;122:e1128–e1135. - PubMed
-
- Darbari A, Sabin KM, Shapiro CN, Schwarz KB. Epidemiology of primary hepatic malignancies in US children. Hepatology. 2003;38:560–566. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
