

HIV Neuroinfection and Alzheimer's Disease: Similarities and Potential Links?
- PMID: 30254568
- PMCID: PMC6141679
- DOI: 10.3389/fncel.2018.00307
HIV Neuroinfection and Alzheimer's Disease: Similarities and Potential Links?
Abstract
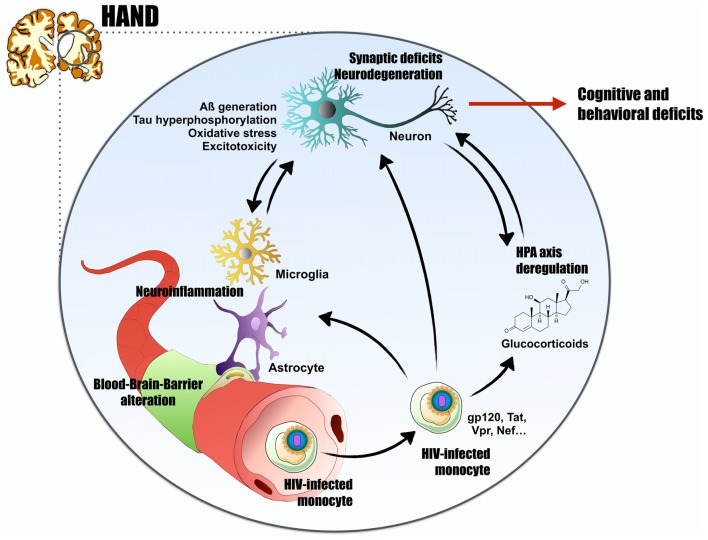
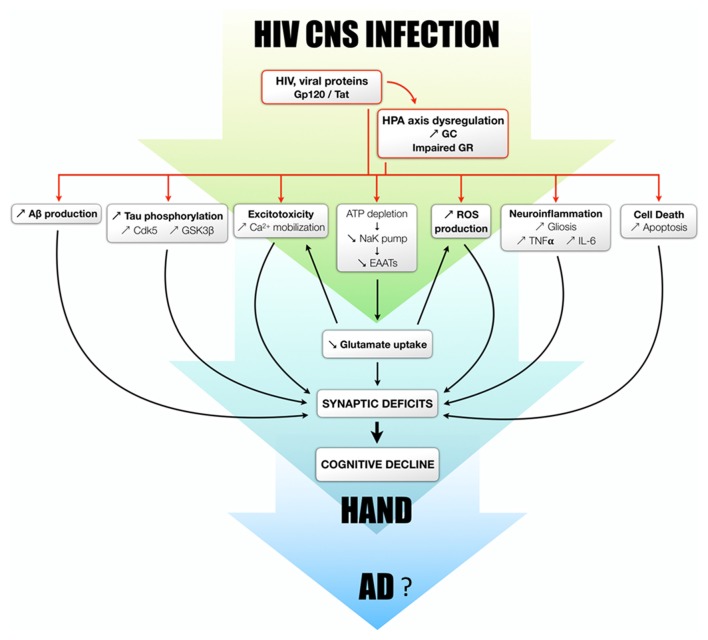
Environmental factors such as chemicals, stress and pathogens are now widely believed to play important roles in the onset of some brain diseases, as they are associated with neuronal impairment and acute or chronic inflammation. Alzheimer's disease (AD) is characterized by progressive synaptic dysfunction and neurodegeneration that ultimately lead to dementia. Neuroinflammation also plays a prominent role in AD and possible links to viruses have been proposed. In particular, the human immunodeficiency virus (HIV) can pass the blood-brain barrier and cause neuronal dysfunction leading to cognitive dysfunctions called HIV-associated neurocognitive disorders (HAND). Similarities between HAND and HIV exist as numerous factors involved in AD such as members of the amyloid and Tau pathways, as well as stress-related pathways or blood brain barrier (BBB) regulators, seem to be modulated by HIV brain infection, leading to the accumulation of amyloid plaques or neurofibrillary tangles (NFT) in some patients. Here, we summarize findings regarding how HIV and some of its proteins such as Tat and gp120 modulate signaling and cellular pathways also impaired in AD, suggesting similarities and convergences of these two pathologies.
Keywords: Alzheimer’s disease; HIV-associated neurocognitive disorders; hypothalamo-pituitary-adrenal axis; neuroinflammation; viral neuroinfection.
Figures
References
-
- Adle-Biassette H., Chrétien F., Wingertsmann L., Héry C., Ereau T., Scaravilli F., et al. (1999). Neuronal apoptosis does not correlate with dementia in HIV infection but is related to microglial activation and axonal damage. Neuropathol. Appl. Neurobiol. 25, 123–133. 10.1046/j.1365-2990.1999.00167.x - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources