

Intracranial Atherosclerosis Versus Primary Angiitis of the Central Nervous System: a Case Report
- PMID: 30254820
- PMCID: PMC6150750
- DOI: 10.7759/cureus.3031
Intracranial Atherosclerosis Versus Primary Angiitis of the Central Nervous System: a Case Report
Abstract
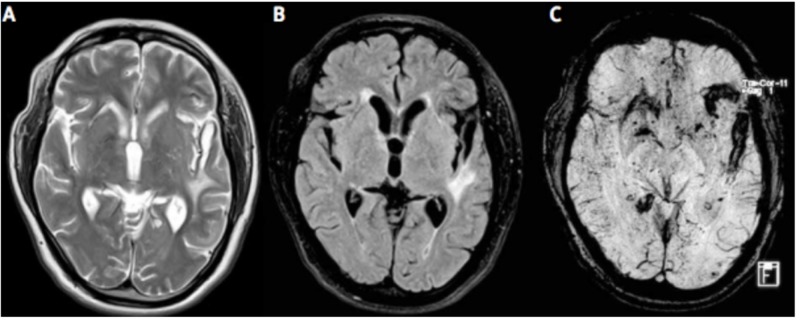
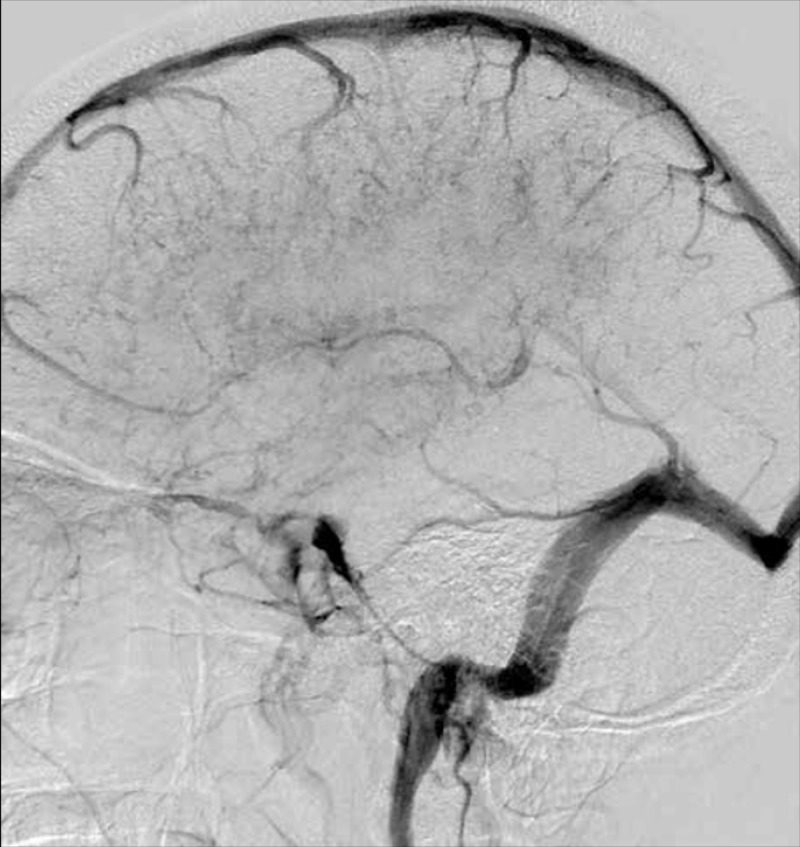
Primary angiitis of the central nervous system (PACNS) is a rare disease with various clinical presentations. It is the preferred name for vasculitis that is confined to the central nervous system (CNS) and is often considered a diagnosis of exclusion in vascular or inflammatory CNS diseases. This case describes a 46-year-old right-handed female with a past medical history of hypertension (HTN), hyperlipidemia (HLD), diabetes mellitus type two (DM2), obesity, and hemorrhagic stroke who was transferred from an outside facility after a one-month hospitalization to be evaluated for CNS vasculitis. Emergency medical personnel who brought the patient to the receiving hospital endorsed dysarthria and fluctuating level of cognition. Before she was transferred, the patient underwent a series of computed tomography (CT) and magnetic resonance imaging and angiographies (MRI/MRA) as well as four-vessel angiography. The studies revealed multiple bilateral striatal and cortical infarcts, scattered narrowing and occlusion of major cerebral vasculature, as well as other signs initially more suggestive of intracranial atherosclerosis than CNS vasculitis. Before she was transferred, imaging demonstrated a new cortical stroke. Hypercoagulable studies were positive for protein C deficiency although ensuing echocardiograms with normal ejection fractions were negative for a source of cardioembolism. Having undergone extensive rheumatological, radiological, and neurosurgical evaluation in the receiving facility, recommendations were made for the patient to undergo leptomeningeal biopsy to confirm the diagnosis of vasculopathy and to specifically rule out intracranial atherosclerosis and reversible cerebral vasoconstriction syndrome (RCVS).
Keywords: cerebral angiography; cns vasculitis; intracranial atherosclerosis; magnetic resonance angiography; primary angiitis of the central nervous system; reversible cerebral vasoconstriction disorder; vasculitis.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Primary Angiitis of the Central Nervous System: An Uncommon Cause of Stroke in the Young.Cureus. 2022 Aug 8;14(8):e27799. doi: 10.7759/cureus.27799. eCollection 2022 Aug. Cureus. 2022. PMID: 36106213 Free PMC article.
-
Reversible cerebral vasoconstriction syndrome or primary angiitis of the central nervous system?Can J Neurol Sci. 2007 Nov;34(4):467-77. Can J Neurol Sci. 2007. PMID: 18062458
-
Reversible Cerebral Vasoconstriction Syndrome without Headache That Was Initially Suspected of Being Primary Angiitis of the Central Nervous System.Intern Med. 2021 Jul 15;60(14):2321-2326. doi: 10.2169/internalmedicine.6560-20. Epub 2021 Feb 22. Intern Med. 2021. PMID: 33612678 Free PMC article.
-
Diagnostic and therapeutic approach to adult central nervous system vasculitis.Rev Neurol (Paris). 2022 Dec;178(10):1041-1054. doi: 10.1016/j.neurol.2022.05.003. Epub 2022 Sep 22. Rev Neurol (Paris). 2022. PMID: 36156251 Review.
-
Primary angiitis of the central nervous system: differential diagnosis and treatment.Best Pract Res Clin Rheumatol. 2010 Jun;24(3):413-26. doi: 10.1016/j.berh.2009.12.003. Best Pract Res Clin Rheumatol. 2010. PMID: 20534374 Review.
Cited by
-
Unraveling cerebrovascular involvement in EGPA through digital subtraction angiography: case presentation and systematic literature review.BMC Rheumatol. 2025 Jul 1;9(1):80. doi: 10.1186/s41927-025-00518-7. BMC Rheumatol. 2025. PMID: 40597425 Free PMC article.
References
-
- Noninfectious granulomatous angiitis with a predilection for the nervous system. [May;2018 ];Cravioto H, Feigin Feigin, I I. Neurology. 1959 9:599–609. - PubMed
-
- Primary angiitis of the central nervous system in adults. [Feb;2018 ];Hajj-Ali , Calabrese Calabrese, LH LH. https://www.uptodate.com/contents/primary-angiitis-of-the-central-nervou... UpToDate. 2017
-
- CNS vasculitis. [Feb;2018 ];John S, Hajj-Ali RA. Semin Neurol. 2014 34:405–412. - PubMed
-
- Primary angiitis of the CNS differential diagnoses. [Feb;2018 ];https://emedicine.medscape.com/article/1484146-differential 2016
-
- Primary angiitis of the central nervous system: a study of histopathological patterns and review of the literature. [Feb;2018 ];Suri V, Kakkar A, Sharma MC. Folia Neuropathol. 2014 52:187–196. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous