Timing for initiation of sequential continuous renal replacement therapy in patients on extracorporeal membrane oxygenation
- PMID: 30254848
- PMCID: PMC6147187
- DOI: 10.23876/j.krcp.2018.37.3.239
Timing for initiation of sequential continuous renal replacement therapy in patients on extracorporeal membrane oxygenation
Abstract
Background: Extracorporeal membrane oxygenation (ECMO) is a lifesaving therapy used in critically ill patients with severe cardiopulmonary dysfunction. Continuous renal replacement therapy (CRRT) is supplemented to treat fluid overload, acute kidney injury, and electrolyte disturbances during ECMO. However, the best time to initiate CRRT is not well-defined. We performed this study to identify the optimal timing of CRRT for ECMO.
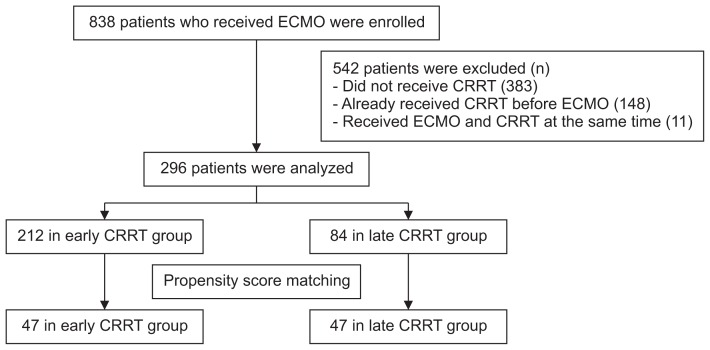
Methods: We conducted a multicenter retrospective cohort study of 296 patients over 12 years. Patients received CRRT during ECMO at Seoul National University Hospital, Seoul National University Bundang Hospital, or Yonsei University Hospital. We assigned patients to an early or late CRRT group depending on the CRRT initiation time. We considered early CRRT to be CRRT instituted within 72 hours of ECMO initiation.
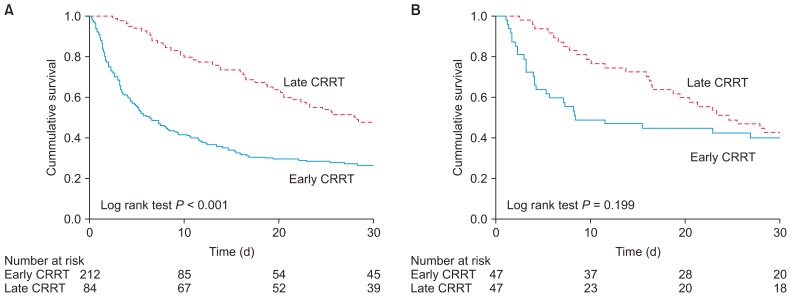
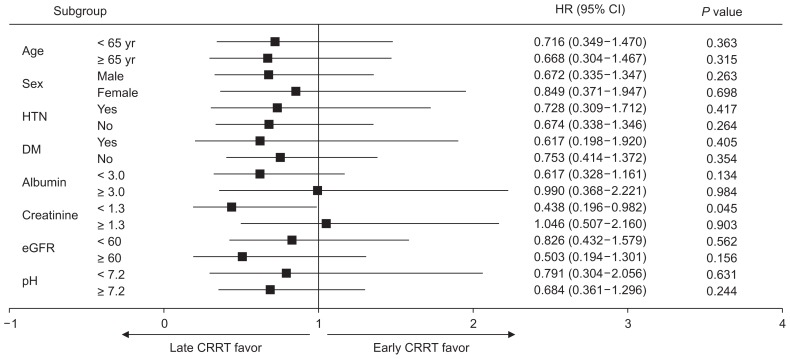
Results: Among 296 patients, 212 patients (71.6%) received early CRRT. After using a propensity score matching method, 47 patients were included in each group. The time from ECMO initiation to CRRT initiation was 1.1 ± 0.9 days in the early CRRT group and 14.6 ± 18.6 days in the late CRRT group. No difference in patients' mortality (P = 0.834) or hospital stay (P = 0.627) between the early and late CRRT groups was found. After adjusting all covariables, there was no significant difference in mortality between the early and late CRRT groups (hazard ratio, 0.697; 95% confidence interval, 0.410-1.184; P = 0.182).
Conclusion: This study showed that early CRRT may not be superior to late CRRT in ECMO patients. Further clinical trials are warranted.
Keywords: Extracorporeal membrane oxygenation; Mortality; Renal replacement therapy; Time-to-treatment.
Conflict of interest statement
Conflicts of interest All authors have no conflicts of interest to declare.
Figures
Similar articles
-
Fluid overload and fluid removal in pediatric patients on extracorporeal membrane oxygenation requiring continuous renal replacement therapy: a multicenter retrospective cohort study.Pediatr Nephrol. 2020 May;35(5):871-882. doi: 10.1007/s00467-019-04468-4. Epub 2020 Jan 17. Pediatr Nephrol. 2020. PMID: 31953749 Free PMC article.
-
Outcomes among Patients Treated with Renal Replacement Therapy during Extracorporeal Membrane Oxygenation: A Single-Center Retrospective Study.Blood Purif. 2020;49(3):341-347. doi: 10.1159/000504287. Epub 2019 Dec 19. Blood Purif. 2020. PMID: 31865351 Free PMC article.
-
Retrospective study on the effects of the prognosis of patients treated with extracorporeal membrane oxygenation combined with continuous renal replacement therapy.Ann Transl Med. 2018 Dec;6(23):455. doi: 10.21037/atm.2018.11.12. Ann Transl Med. 2018. PMID: 30603643 Free PMC article.
-
Continuous renal replacement therapy in patients treated with extracorporeal membrane oxygenation.Semin Dial. 2021 Nov;34(6):537-549. doi: 10.1111/sdi.12965. Epub 2021 Mar 25. Semin Dial. 2021. PMID: 33765346 Free PMC article. Review.
-
Managing the kidney - The role of continuous renal replacement therapy in neonatal and pediatric ECMO.Semin Pediatr Surg. 2023 Aug;32(4):151332. doi: 10.1016/j.sempedsurg.2023.151332. Epub 2023 Oct 17. Semin Pediatr Surg. 2023. PMID: 37871460 Review.
Cited by
-
Acute kidney injury in ECMO patients.Crit Care. 2021 Aug 31;25(1):313. doi: 10.1186/s13054-021-03676-5. Crit Care. 2021. PMID: 34461966 Free PMC article. Review.
-
Nursing effect of ECMO combined with CRRT in the treatment of fulminant myocarditis: A protocol of randomized controlled trial.Medicine (Baltimore). 2021 Jan 22;100(3):e24085. doi: 10.1097/MD.0000000000024085. Medicine (Baltimore). 2021. PMID: 33546013 Free PMC article.
-
Impact of early initiation of renal replacement therapy in patients on venoarterial ECMO using target trial emulation with Japanese nationwide data.Sci Rep. 2025 Jan 7;15(1):1074. doi: 10.1038/s41598-025-85109-9. Sci Rep. 2025. PMID: 39774191 Free PMC article.
-
Renal replacement therapy during extracorporeal membrane oxygenation.Indian J Thorac Cardiovasc Surg. 2021 Apr;37(Suppl 2):261-266. doi: 10.1007/s12055-019-00920-0. Epub 2020 Jan 29. Indian J Thorac Cardiovasc Surg. 2021. PMID: 33967450 Free PMC article. Review.
-
Kidney replacement therapy during extracorporeal membrane oxygenation: pathophysiology, technical considerations, and outcomes.Ren Fail. 2025 Dec;47(1):2486557. doi: 10.1080/0886022X.2025.2486557. Epub 2025 Apr 23. Ren Fail. 2025. PMID: 40265202 Free PMC article. Review.
References
-
- Peek GJ, Mugford M, Tiruvoipati R, et al. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicentre randomised controlled trial. Lancet. 2009;374:1351–1363. doi: 10.1016/S0140-6736(09)61069-2. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical