

Expectant management for abdominal pregnancy
- PMID: 30254883
- PMCID: PMC6113971
- DOI: 10.1016/j.gmit.2016.11.003
Expectant management for abdominal pregnancy
Abstract
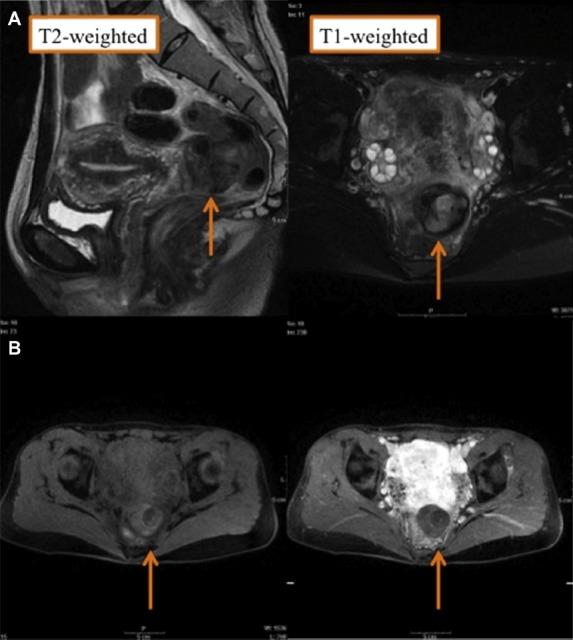
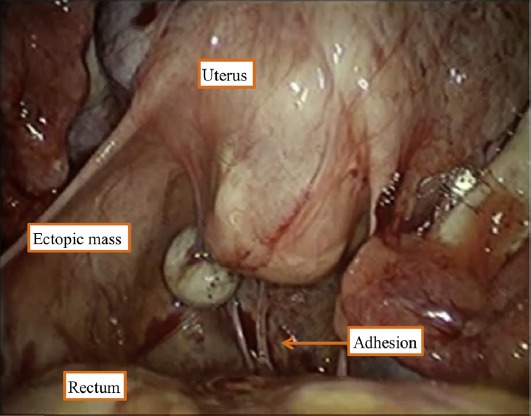
This is the first English language report describing the expectant management for abdominal pregnancy. The patient was a 31-year-old multiparous woman who was transferred to our hospital on suspicion of ectopic pregnancy. Her serum human chorionic gonadotropin was positive, and a poorly-vascularized mass measuring about 4 cm was visualized in the Douglas pouch by transvaginal ultrasonography, as well as by pelvic magnetic resonance imaging. Because the bilateral adnexa were apparently intact, she was diagnosed with abdominal pregnancy, and expectant management was commenced. Unexpectedly, the mass remained in situ for nearly 3 years after her serum human chorionic gonadotropin tested negative. Laparoscopic removal of the mass was finally required because of persistent defecation pain. This case illustrates that some abdominal pregnancies can be managed expectantly, as is the case with tubal pregnancies. During the expectant management, however, it should be considered that the abdominal pregnancy mass may persist for a longer period and cause moderate symptoms necessitating surgical removal.
Keywords: MRI; defecation pain; ectopic pregnancy; laparoscopy; transvaginal ultrasonography.
Conflict of interest statement
Conflicts of interest: The authors have no conflicts of interest relevant to this article.
Figures
References
-
- Atrash HK, Friede A, Hogue CJ. Abdominal pregnancy in the United States: frequency and maternal mortality. Obstet Gynecol. 1987;69(3 Pt 1):333–337. - PubMed
-
- Dover RW, Powell MC. Management of a primary abdominal pregnancy. Am J Obstet Gynecol. 1995;172:1603–1604. - PubMed
-
- Ginath S, Malinger G, Golan A, Shahmurov M, Glezerman M. Successful laparoscopic treatment of a ruptured primary abdominal pregnancy. Fertil Steril. 2000;74:601–602. - PubMed
-
- Varma R, Mascarenhas L, James D. Successful outcome of advanced abdominal pregnancy with exclusive omental insertion. Ultrasound Obstet Gynecol. 2003;21:192–194. - PubMed
-
- Kitade M, Takeuchi H, Kikuchi I, Shimanuki H, Kumakiri J, Kinoshita K. A case of simultaneous tubal-splenic pregnancy after assisted reproductive technology. Fertil Steril. 2005;83:1042. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources