

Initial closed trocar entry for laparoscopic surgery: Technique, umbilical cosmesis, and patient satisfaction
- PMID: 30254907
- PMCID: PMC6135191
- DOI: 10.1016/j.gmit.2017.04.001
Initial closed trocar entry for laparoscopic surgery: Technique, umbilical cosmesis, and patient satisfaction
Abstract
Background/aims: Despite the benefits of laparoscopic surgery, which is being performed with increasing frequency, complications that do not occur during laparotomy are sometimes encountered. Such complications commonly occur during the initial trocar insertion, making this a procedural step of critical importance.
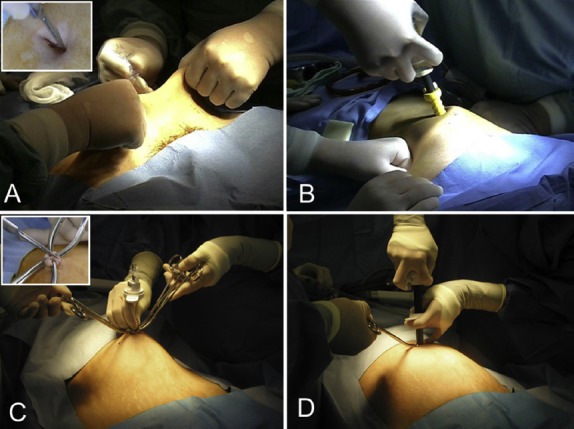
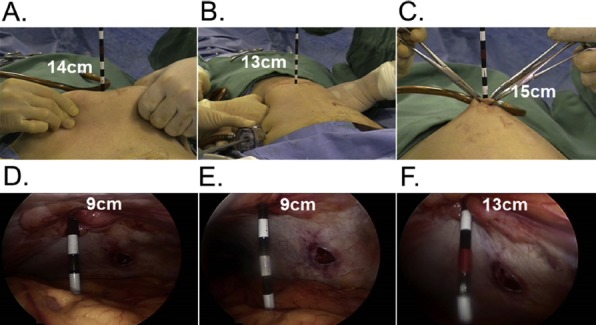
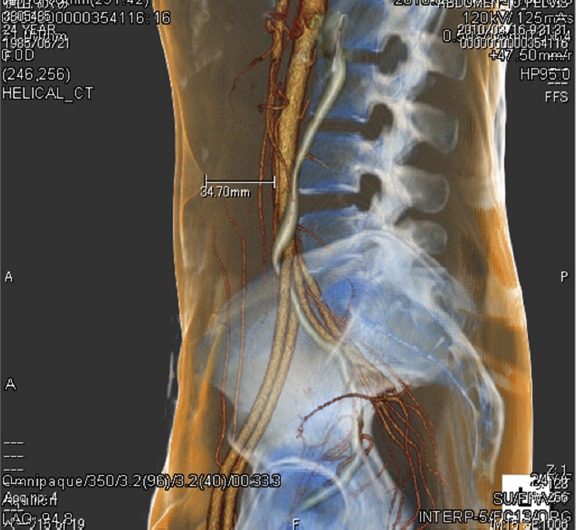
Methods: In 2002, we experienced, upon initial trocar insertion, a serious major vascular injury (MVI) that led to hemorrhagic shock, and we thus modified the conventional closed entry method to an approach that we have found to be safe. We began developing the method by first measuring, in a patient undergoing laparoscopic cystectomy, the distance between the inner surface of the abdominal wall and the anterior spine when the abdominal wall was lifted manually for trocar insertion and when it was lifted by other methods, and we determined which method provided the greatest distance. We then devised a new approach, summarized as follows: The umbilical ring is elevated with Kocher forceps. The umbilicus is everted, and the base is incised longitudinally. This allows penetration of the abdominal wall at its thinnest point, and it shortens the distance to the abdominal cavity. A bladeless trocar (Step trocar) is used to allow insertion of the Veress needle. We began applying the new entry technique in July 2002, and by December 2014, we had applied it to 9676 patients undergoing laparoscopic gynecology surgery.
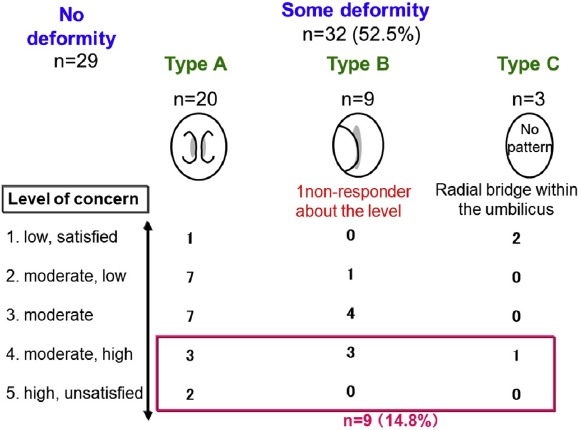
Results: All entries were performed successfully, and no MVI occurred. The umbilical incision often resulted in an umbilical deformity, but in a questionnaire-based survey, patients generally reported satisfaction with the cosmetic outcome.
Conclusion: A current new approach provides safe outcome with a minor cosmetic problem.
Keywords: Closed laparoscopy; Laparoscopic myomectomy; Major vascular injury; Umbilical deformity.
Conflict of interest statement
Conflicts of interest statement: The authors have no conflicts of interest relevant to this article.
Figures

References
-
- Peterson HB, Hulka JF, Phillips JM, Surrey MW. Laparoscopic sterilization. American Association of Gynecologic Laparoscopists' 1991 membership survey. J Reprod Med. 1993;38:574–576. - PubMed
-
- Munro MG. Laparoscopic access: complications, technologies and techniques. Curr Opin Obstet Gynecol. 2002;4:365–374. - PubMed
-
- Nuzzo G, Giuliante F, Tebala GD, Vellone M, Cavicchioni C. Routine use of open technique in laparoscopic operations. J Am Coll Surg. 1997;184:58–62. - PubMed
-
- Bonjer HJ, Hazebroek EJ, Kazemier G, Giuffrida MC, Meijer WS, Lange JF. Open versus closed establishment of pneumoperitoneum in laparoscopy surgery. Br J Surg. 1997;84:599–602. - PubMed
-
- Roy GM, Bazzurini L, Solima E, Luciano AA. Safe technique for laparoscopic entry into the abdominal cavity. J Am Assoc Gynecol Laparosc. 2001;8:519–528. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources