

Breast density implications and supplemental screening
- PMID: 30255244
- PMCID: PMC6420861
- DOI: 10.1007/s00330-018-5668-8
Breast density implications and supplemental screening
Abstract
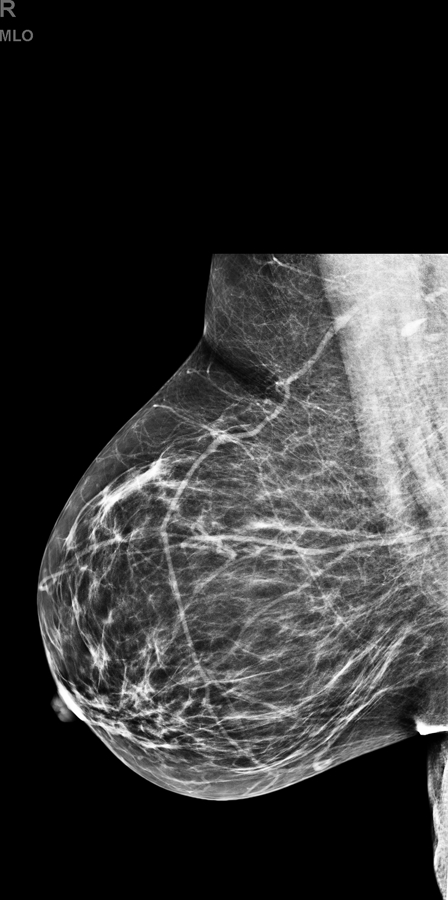
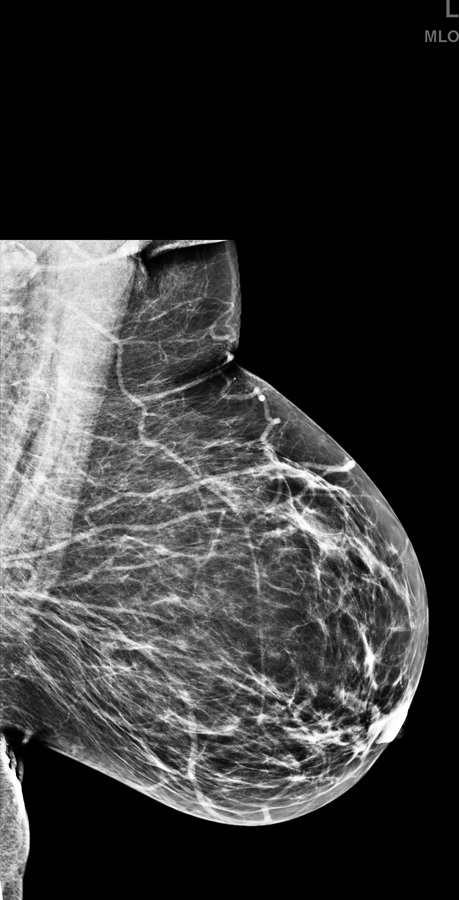
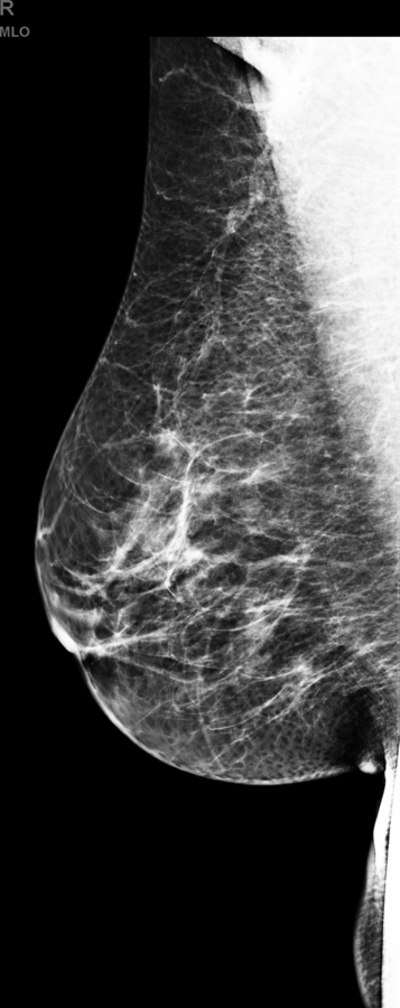
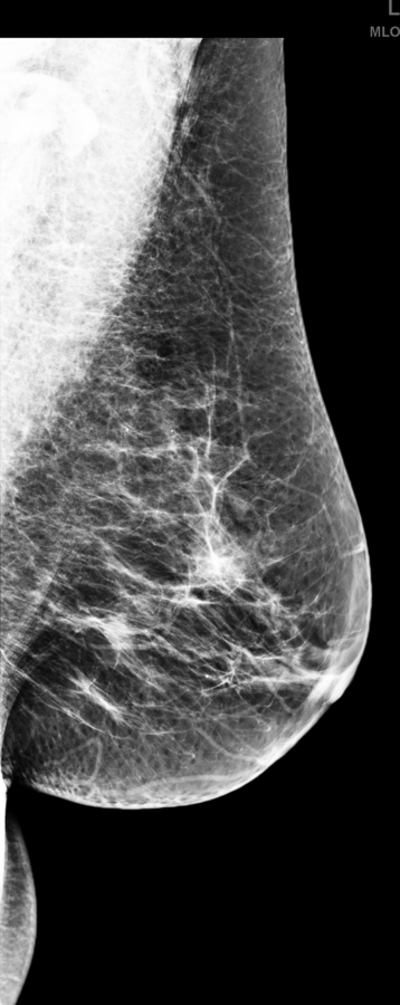
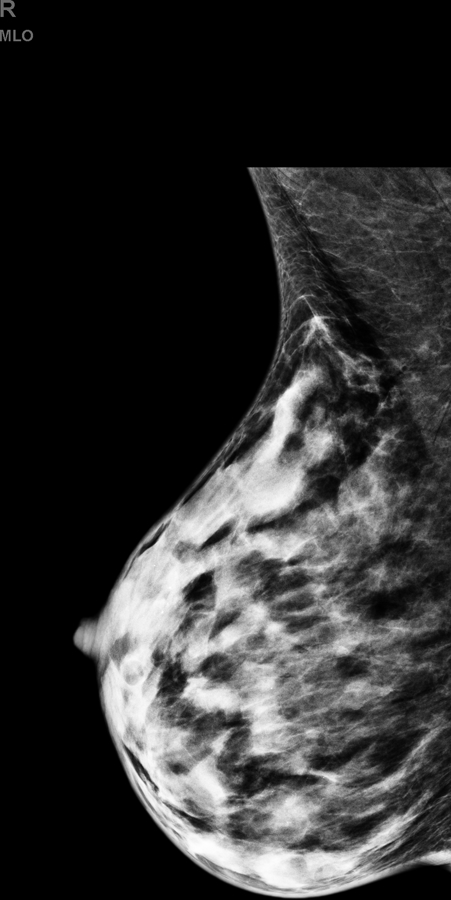
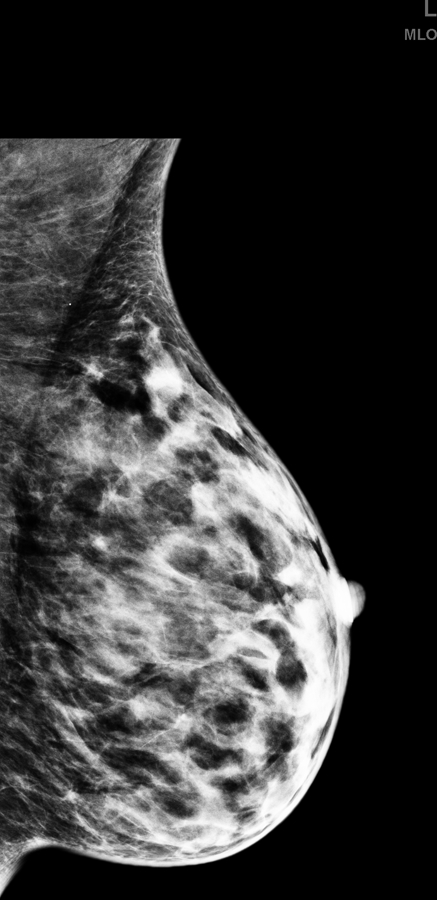
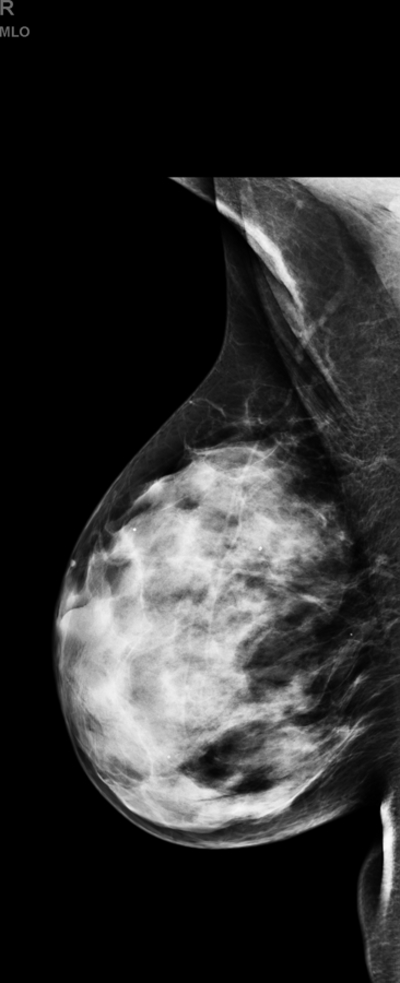
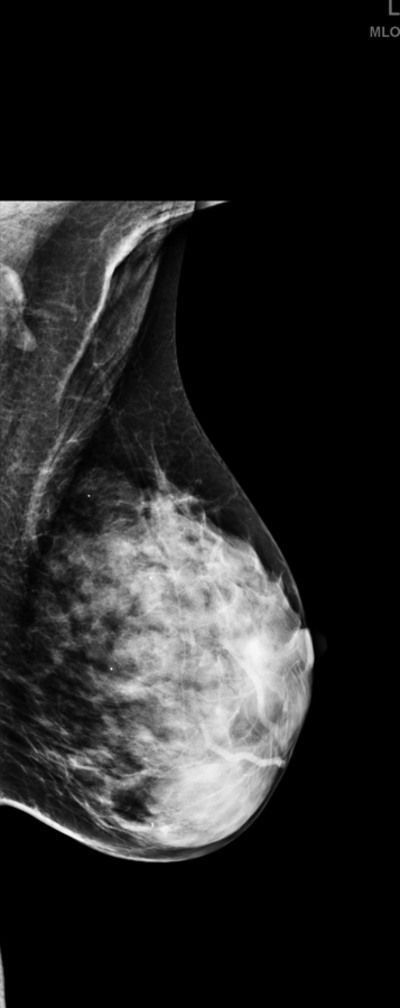
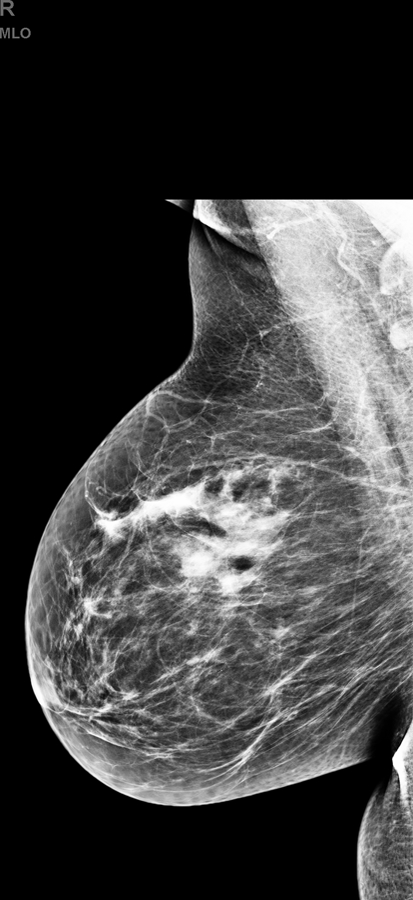
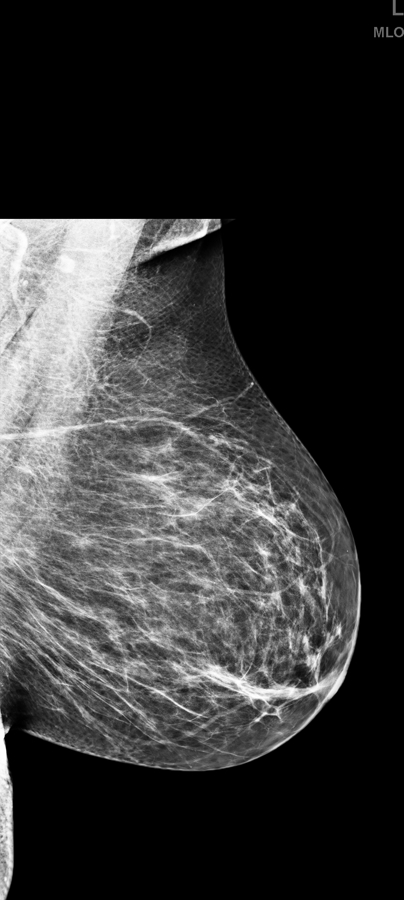
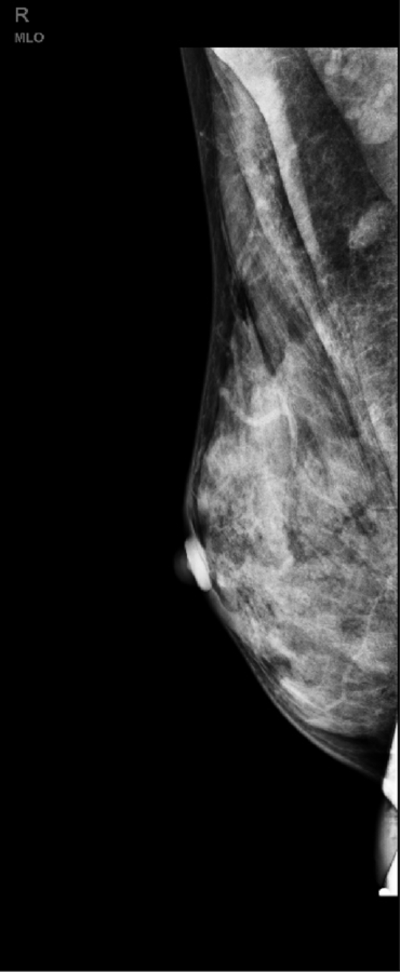
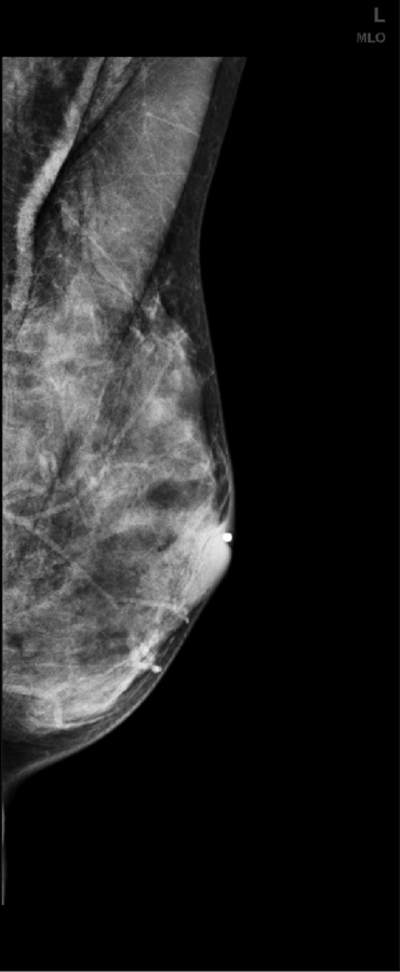
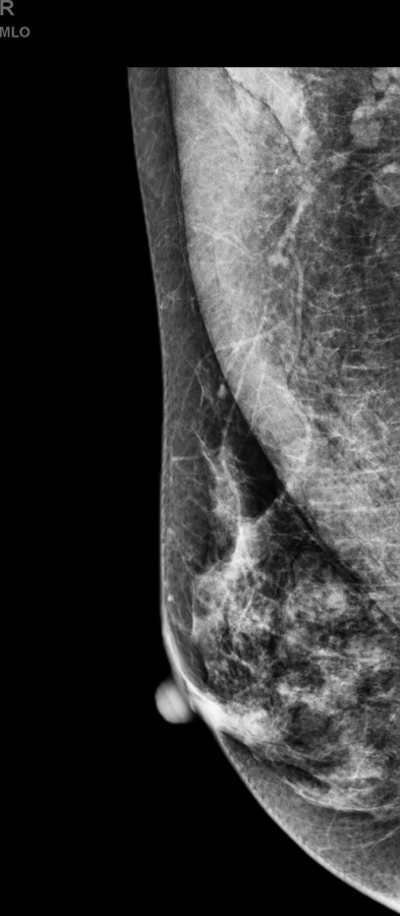
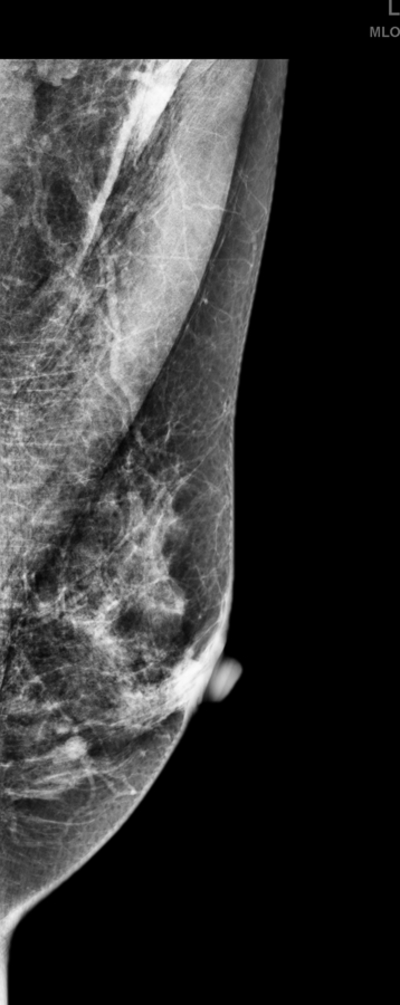
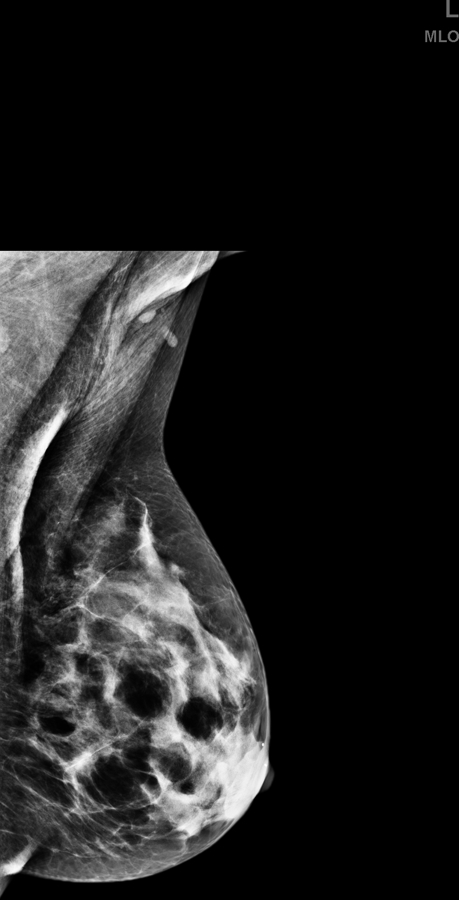
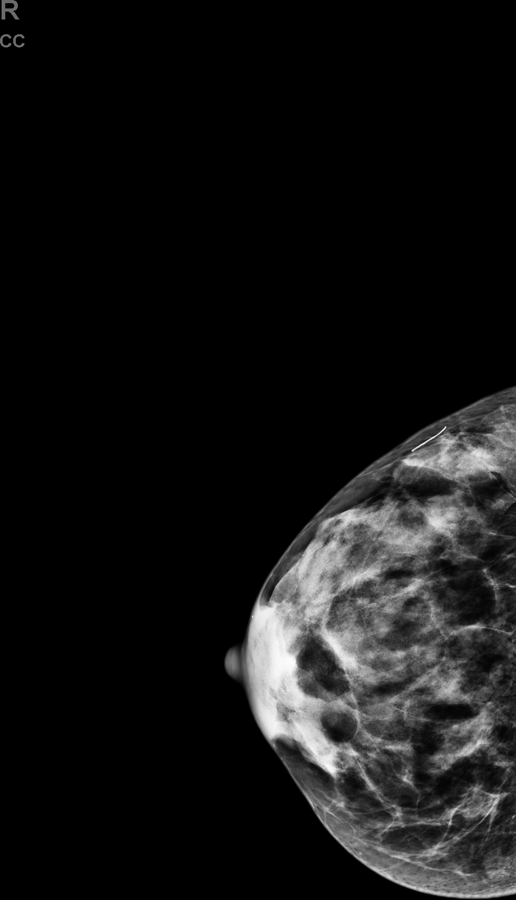
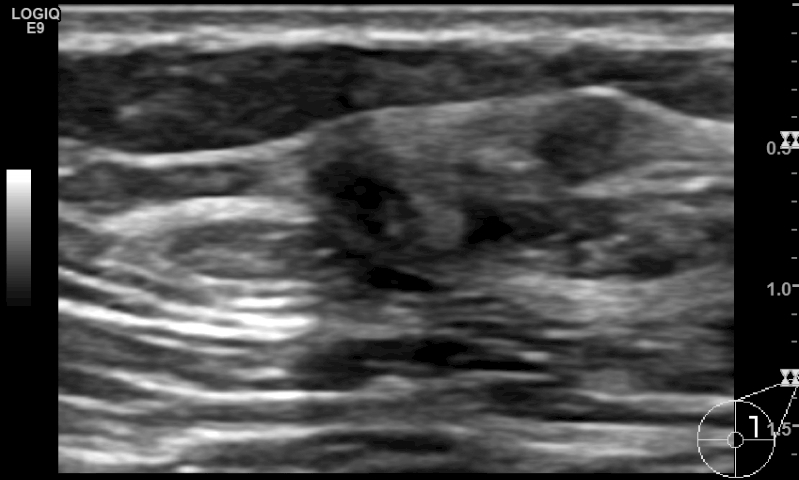
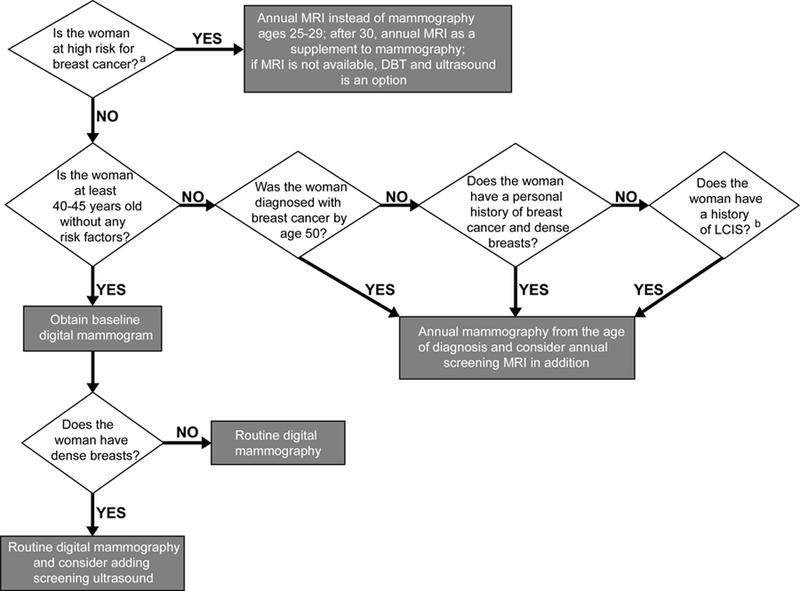
Digital breast tomosynthesis (DBT) has been widely implemented in place of 2D mammography, although it is less effective in women with extremely dense breasts. Breast ultrasound detects additional early-stage, invasive breast cancers when combined with mammography; however, its relevant limitations, including the shortage of trained operators, operator dependence and small field of view, have limited its widespread implementation. Automated breast sonography (ABS) is a promising technique but the time to interpret and false-positive rates need to be improved. Supplemental screening with contrast-enhanced magnetic resonance imaging (MRI) in high-risk women reduces late-stage disease; abbreviated MRI protocols may reduce cost and increase accessibility to women of average risk with dense breasts. Contrast-enhanced digital mammography (CEDM) and molecular breast imaging improve cancer detection but require further validation for screening and direct biopsy guidance should be implemented for any screening modality. This article reviews the status of screening women with dense breasts. KEY POINTS: • The sensitivity of mammography is reduced in women with dense breasts. Supplemental screening with US detects early-stage, invasive breast cancers. • Tomosynthesis reduces recall rate and increases cancer detection rate but is less effective in women with extremely dense breasts. • Screening MRI improves early diagnosis of breast cancer more than ultrasound and is currently recommended for women at high risk. Risk assessment is needed, to include breast density, to ascertain who should start early annual MRI screening.
Keywords: Breast cancer; Breast density; Magnetic resonance imaging; Screening ultrasound; Tomosynthesis.
Conflict of interest statement
Figures


References
-
- Tabar L, Vitak B, Chen TH et al. (2011) Swedish two-county trial: impact of mammographic screening on breast cancer mortality during 3 decades. Radiology 260:658–663. - PubMed
-
- Coldman A, Phillips N, Wilson C et al. (2014) Pan-Canadian study of mammography screening and mortality from breast cancer. J Natl Cancer Inst 106. - PubMed
-
- Broeders M, Moss S, Nystrom L et al. (2012) The impact of mammographic screening on breast cancer mortality in Europe: a review of observational studies. J Med Screen 19 Suppl 1:14–25. - PubMed
-
- Tabar L, Yen AM, Wu WY et al. (2015) Insights from the breast cancer screening trials: how screening affects the natural history of breast cancer and implications for evaluating service screening programs. Breast J 21:13–20. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
