

Serum testosterone, sex hormone-binding globulin and sex-specific risk of incident type 2 diabetes in a retrospective primary care cohort
- PMID: 30256433
- PMCID: PMC6334272
- DOI: 10.1111/cen.13862
Serum testosterone, sex hormone-binding globulin and sex-specific risk of incident type 2 diabetes in a retrospective primary care cohort
Abstract
Objective: Previous studies suggest that androgens have a sexually dimorphic impact on metabolic dysfunction. However, the sex-specific link between circulating androgens and risk of type 2 diabetes mellitus (T2DM) has not been examined in a large scale, longitudinal cohort, a task we undertook in this study.
Design: A retrospective cohort study in a UK primary care database.
Patients: We included men and women with available serum testosterone and sex hormone-binding globulin (SHBG) results.
Measurements: We categorized serum concentrations according to clinically relevant cut-off points and calculated crude and adjusted T2DM Incidence Rate Ratios (IRRs and aIRRs).
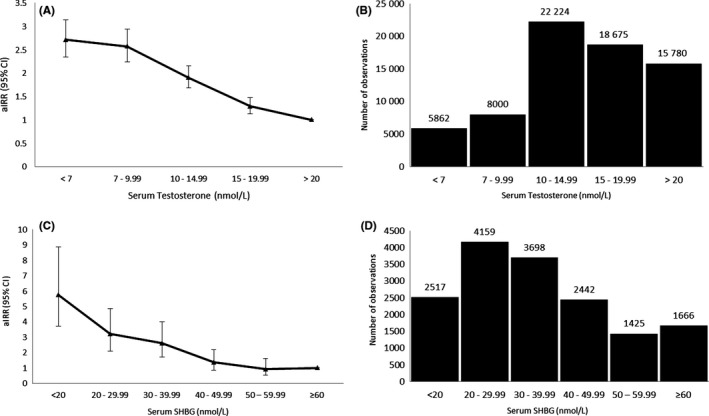
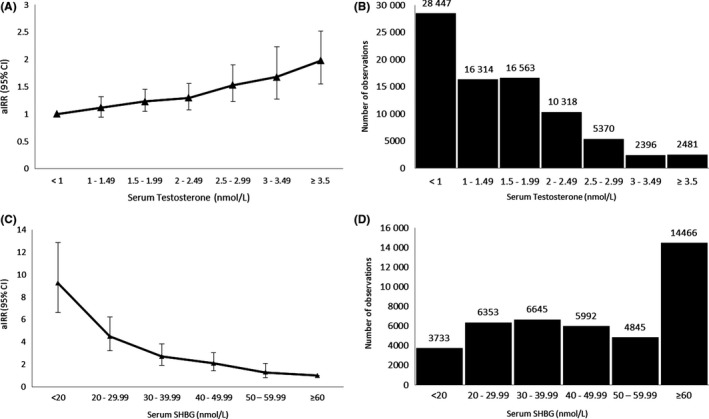
Results: Serum testosterone concentrations were available in 70 541 men and 81 889 women; serum SHBG was available in 15 907 men and 42 034 women. In comparison to a reference cohort with serum testosterone ≥20 nmol/L, men with lower serum testosterone had a significantly increased risk of T2DM, with the highest risk in those with serum testosterone <7 nmol/L (aIRR 2.71, 95% CI 2.34-3.14, P < 0.001). In women, the risk of T2DM started to increase significantly when serum testosterone concentrations exceeded 1.5 nmol/L, with the highest risk in women with serum testosterone ≥3.5 nmol/L (aIRR 1.98, 95% CI 1.55-2.52, P < 0.001). These observations were verified in a continuous rather than categorized analysis. The risk of T2DM increased in men and women with serum SHBG <40 and <50 nmol/L, respectively.
Conclusions/interpretation: In this longitudinal study, we found sexually dimorphic associations between serum testosterone and risk of incident T2DM. Androgen deficiency and excess should be considered important risk factors for diabetes in men and women, respectively.
Keywords: androgens; diabetes; hypogonadism; metabolic diseases; population health; sex hormone-binding globulin; testosterone.
© 2018 The Authors Clinical Endocrinology Published by John Wiley & Sons Ltd.
Figures
References
-
- Maraka S, Singh Ospina N, Rodriguez‐Gutierrez R, et al. Sex steroids and cardiovascular outcomes in transgender individuals: a systematic review and meta‐analysis. J Clin Endocrinol Metab. 2017;102(11):3914‐3923. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
