

Hypocapnic cerebral hypoperfusion: A biomarker of orthostatic intolerance
- PMID: 30256820
- PMCID: PMC6157889
- DOI: 10.1371/journal.pone.0204419
Hypocapnic cerebral hypoperfusion: A biomarker of orthostatic intolerance
Abstract
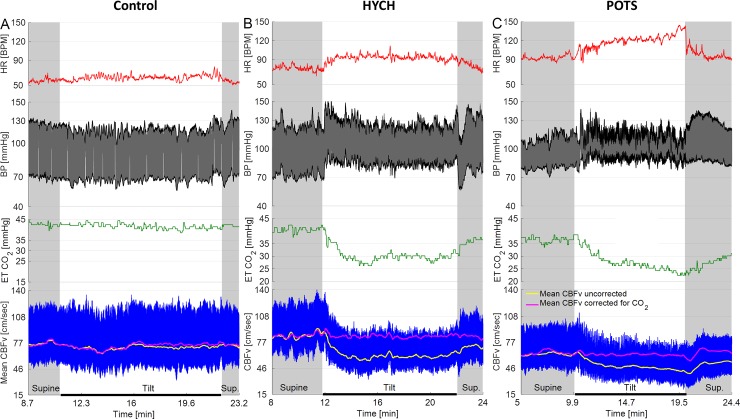
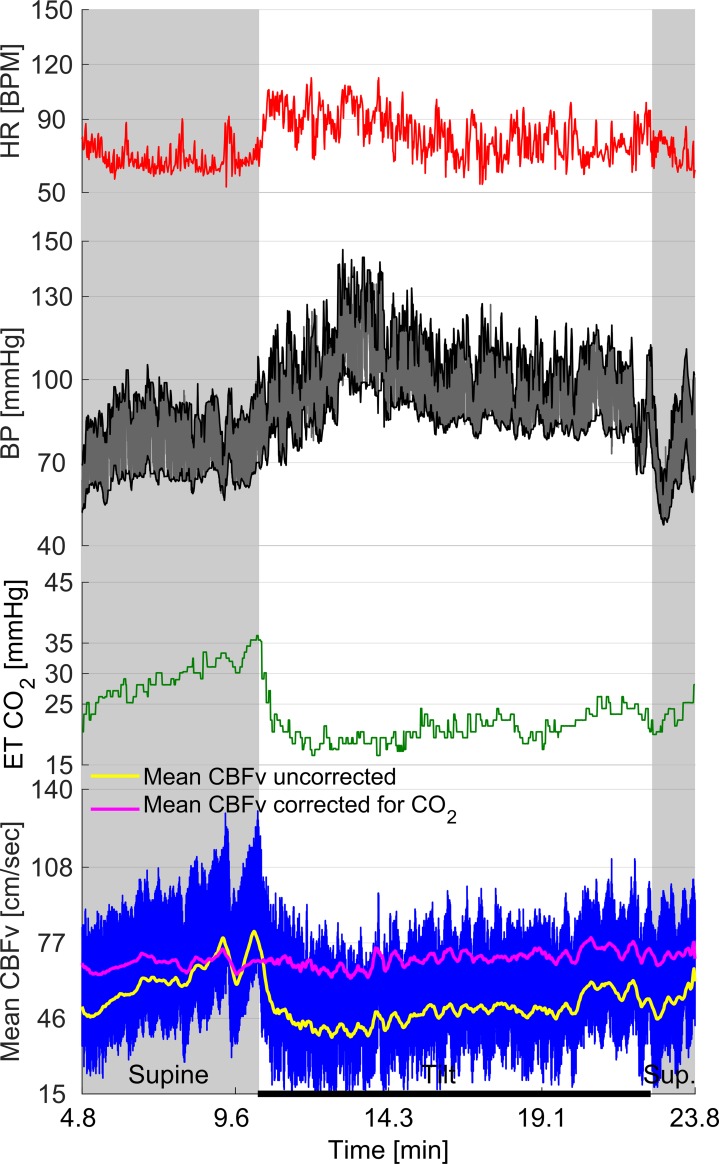
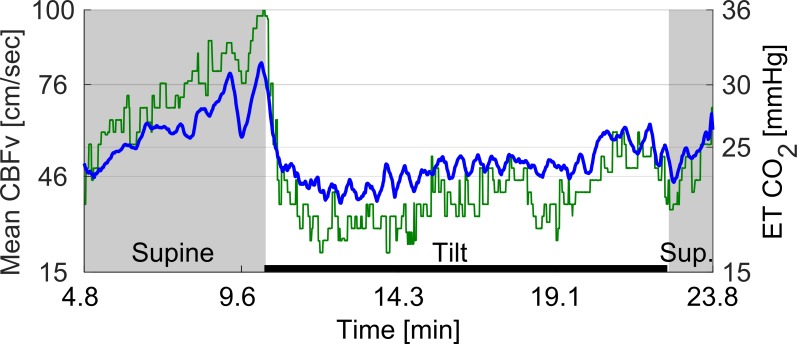
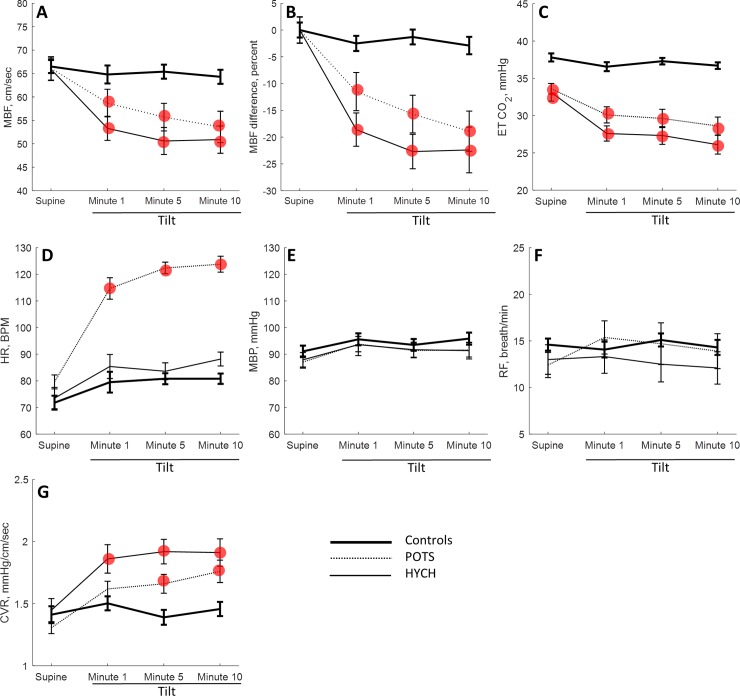
The objective of the study was to identify markers of hypocapnic cerebral hypoperfusion (HYCH) in patients with orthostatic intolerance (OI) without tachycardia and without orthostatic hypotension. This single center, retrospective study included OI patients referred for autonomic evaluation with the 10 min tilt test. Heart rate, end-tidal CO2 (ET-CO2), blood pressure, and cerebral blood flow velocity (CBFv) from middle cerebral artery were monitored. HYCH was defined by: (1) Symptoms of OI; (2) Orthostatic hypocapnia (low ET-CO2); (3) Abnormal decline in orthostatic CBFv due to hypocapnia; 4) Absence of tachycardia, orthostatic hypotension, or other causes of low CBFv or hypocapnia. Sixteen subjects met HYCH criteria (15/1 women/men, age 38.5±8.0 years) and were matched by age and gender to postural tachycardia patients (POTS, n = 16) and healthy controls (n = 16). During the tilt, CBFv decreased more in HYCH (-22.4±7.7%, p<0.0001) and POTS (-19.0±10.3%, p<0.0001) compared to controls (-3.0±5.0%). Orthostatic ET-CO2 was lower in HYCH (26.4±4.2 (mmHg), p<0.0001) and POTS (28.6±4.3, p<0.0001) compared to controls (36.9 ± 2.1 mmHg). Orthostatic heart rate was normal in HYCH (89.0±10.9 (BPM), p<0.08) and controls (80.8 ±11.2), but was higher in POTS (123.7±11.2, p<0.0001). Blood pressure was normal and similar in all groups. It is concluded that both HYCH and POTS patients have comparable decrease in CBFv which is due to vasoconstrictive effect of hypocapnia. Blood flow velocity monitoring can provide an objective biomarker for HYCH in OI patients without tachycardia.
Conflict of interest statement
The author has declared that no competing interests exist.
Figures
Similar articles
-
Orthostatic intolerance with tachycardia (postural tachycardia syndrome) and without (hypocapnic cerebral hypoperfusion) represent a spectrum of the same disorder.Front Neurol. 2024 Oct 30;15:1476918. doi: 10.3389/fneur.2024.1476918. eCollection 2024. Front Neurol. 2024. PMID: 39544990 Free PMC article.
-
Hypocapnia and cerebral hypoperfusion in orthostatic intolerance.Stroke. 1998 Sep;29(9):1876-81. doi: 10.1161/01.str.29.9.1876. Stroke. 1998. PMID: 9731612
-
Cerebral blood flow and end-tidal CO2 predict lightheadedness during head-up tilt in patients with orthostatic intolerance.Neurol Sci. 2024 Dec;45(12):5771-5778. doi: 10.1007/s10072-024-07673-8. Epub 2024 Jul 9. Neurol Sci. 2024. PMID: 38980457
-
Cerebral Blood Flow in Orthostatic Intolerance.J Am Heart Assoc. 2025 Feb 4;14(3):e036752. doi: 10.1161/JAHA.124.036752. Epub 2025 Feb 3. J Am Heart Assoc. 2025. PMID: 39895557 Free PMC article. Review.
-
Cerebrovascular regulation in the postural orthostatic tachycardia syndrome (POTS).Am J Med Sci. 1999 Feb;317(2):124-33. doi: 10.1097/00000441-199902000-00007. Am J Med Sci. 1999. PMID: 10037116 Review.
Cited by
-
Cerebral blood flow remains reduced after tilt testing in myalgic encephalomyelitis/chronic fatigue syndrome patients.Clin Neurophysiol Pract. 2021 Sep 23;6:245-255. doi: 10.1016/j.cnp.2021.09.001. eCollection 2021. Clin Neurophysiol Pract. 2021. PMID: 34667909 Free PMC article.
-
Worsening Symptoms Is Associated with Larger Cerebral Blood Flow Abnormalities during Tilt-Testing in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS).Medicina (Kaunas). 2023 Dec 12;59(12):2153. doi: 10.3390/medicina59122153. Medicina (Kaunas). 2023. PMID: 38138257 Free PMC article.
-
Cardiovascular Autonomic Regulation, ETCO2 and the Heart Rate Response to the Tilt Table Test in Patients with Orthostatic Intolerance.Appl Psychophysiol Biofeedback. 2022 Jun;47(2):107-119. doi: 10.1007/s10484-022-09536-4. Epub 2022 Feb 16. Appl Psychophysiol Biofeedback. 2022. PMID: 35171410
-
Orthostatic Intolerance in Long-Haul COVID after SARS-CoV-2: A Case-Control Comparison with Post-EBV and Insidious-Onset Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Patients.Healthcare (Basel). 2022 Oct 17;10(10):2058. doi: 10.3390/healthcare10102058. Healthcare (Basel). 2022. PMID: 36292504 Free PMC article.
-
Mismatch between subjective and objective dysautonomia.Sci Rep. 2024 Jan 30;14(1):2513. doi: 10.1038/s41598-024-52368-x. Sci Rep. 2024. PMID: 38291116 Free PMC article.
References
-
- Novak V, Spies JM, Novak P, McPhee BR, Rummans TA, Low PA. Hypocapnia and cerebral hypoperfusion in orthostatic intolerance. Stroke. 1998;29: 1876–1881. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
