

Symptomatic Cryptococcal Antigenemia Presenting as Early Cryptococcal Meningitis With Negative Cerebral Spinal Fluid Analysis
- PMID: 30256903
- PMCID: PMC6541705
- DOI: 10.1093/cid/ciy817
Symptomatic Cryptococcal Antigenemia Presenting as Early Cryptococcal Meningitis With Negative Cerebral Spinal Fluid Analysis
Abstract
Background: Individuals with cryptococcal antigenemia are at high risk of developing cryptococcal meningitis if untreated. The progression and timing from asymptomatic infection to cryptococcal meningitis is unclear. We describe a subpopulation of individuals with neurologic symptomatic cryptococcal antigenemia but negative cerebral spinal fluid (CSF) studies.
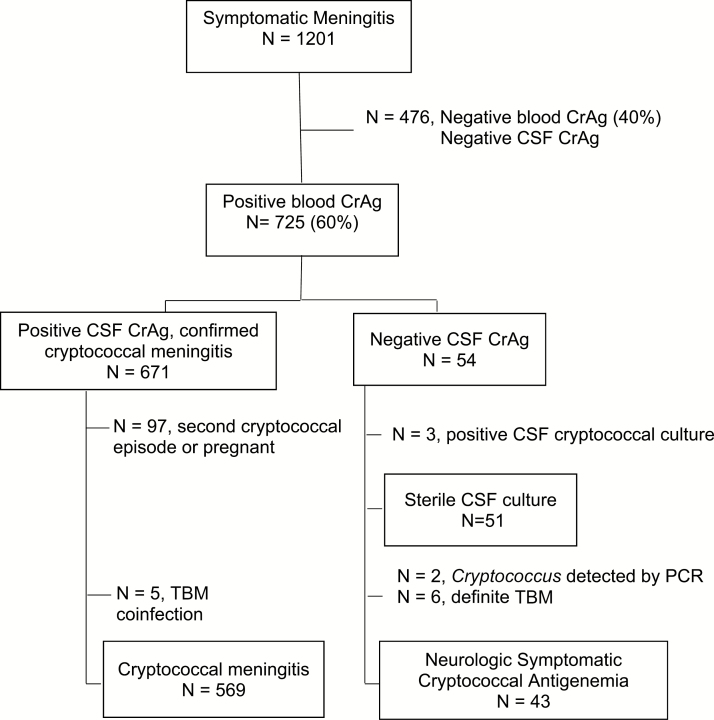
Methods: We evaluated 1201 human immunodeficiency virus-seropositive individuals hospitalized with suspected meningitis in Kampala and Mbarara, Uganda. Baseline characteristics and clinical outcomes of participants with neurologic-symptomatic cryptococcal antigenemia and negative CSF cryptococcal antigen (CrAg) were compared to participants with confirmed CSF CrAg+ cryptococcal meningitis. Additional CSF testing included microscopy, fungal culture, bacterial culture, tuberculosis culture, multiplex FilmArray polymerase chain reaction (PCR; Biofire), and Xpert MTB/Rif.
Results: We found 56% (671/1201) of participants had confirmed CSF CrAg+ cryptococcal meningitis and 4% (54/1201) had neurologic symptomatic cryptococcal antigenemia with negative CSF CrAg. Of those with negative CSF CrAg, 9% (5/54) had Cryptococcus isolated on CSF culture (n = 3) or PCR (n = 2) and 11% (6/54) had confirmed tuberculous meningitis. CSF CrAg-negative patients had lower proportions with CSF pleocytosis (16% vs 26% with ≥5 white cells/μL) and CSF opening pressure >200 mmH2O (16% vs 71%) compared with CSF CrAg-positive patients. No cases of bacterial or viral meningitis were detected by CSF PCR or culture. In-hospital mortality was similar between symptomatic cryptococcal antigenemia (32%) and cryptococcal meningitis (31%; P = .91).
Conclusions: Cryptococcal antigenemia with meningitis symptoms was the third most common meningitis etiology. We postulate this is early cryptococcal meningoencephalitis. Fluconazole monotherapy was suboptimal despite Cryptococcus-negative CSF. Further studies are warranted to understand the clinical course and optimal management of this distinct entity.
Clinical trials registration: NCT01802385.
Keywords: HIV; aseptic meningitis; cryptococcal meningitis; diagnosis; fungal antigen.
© The Author(s) 2018. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
Comment in
-
Detection of Cryptococcus DNA by Metagenomic Next-generation Sequencing in Symptomatic Cryptococcal Antigenemia.Clin Infect Dis. 2019 May 17;68(11):1978-1979. doi: 10.1093/cid/ciy1024. Clin Infect Dis. 2019. PMID: 30535266 Free PMC article. No abstract available.
-
Neurologic Symptomatic Cryptococcal Antigenaemia in a Patient With Well-controlled Human Immunodeficiency Virus.Clin Infect Dis. 2020 Mar 17;70(7):1521-1522. doi: 10.1093/cid/ciz658. Clin Infect Dis. 2020. PMID: 31312835 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
