

Evaluation of Frailty as an Unmeasured Confounder in Observational Studies of Antidiabetic Medications
- PMID: 30256914
- PMCID: PMC6625595
- DOI: 10.1093/gerona/gly224
Evaluation of Frailty as an Unmeasured Confounder in Observational Studies of Antidiabetic Medications
Abstract
Background: It is unknown whether observational studies evaluating the association between antidiabetic medications and mortality adequately account for frailty. Our objectives were to evaluate if frailty was a potential confounder in the relationship between antidiabetic medication regimen and mortality and how well administrative and clinical electronic health record (EHR) data account for frailty.
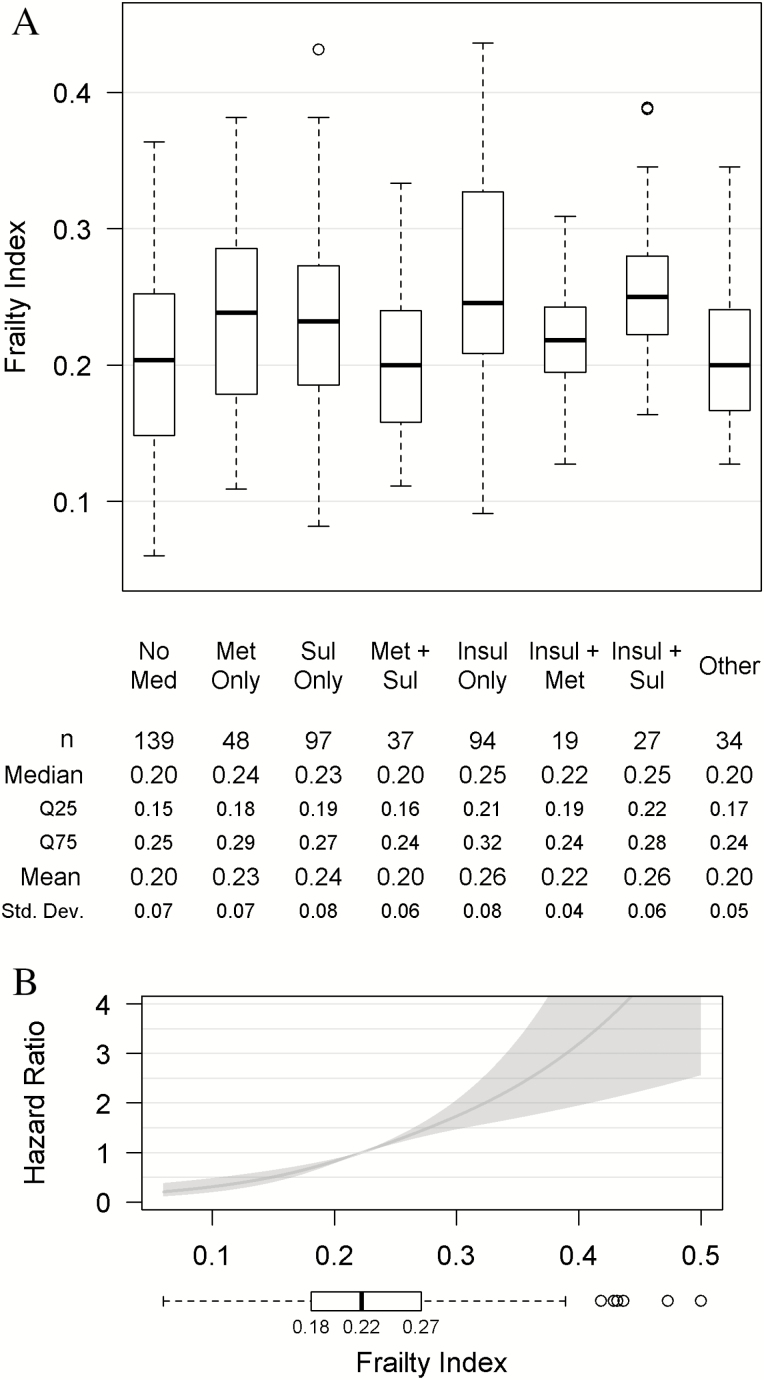
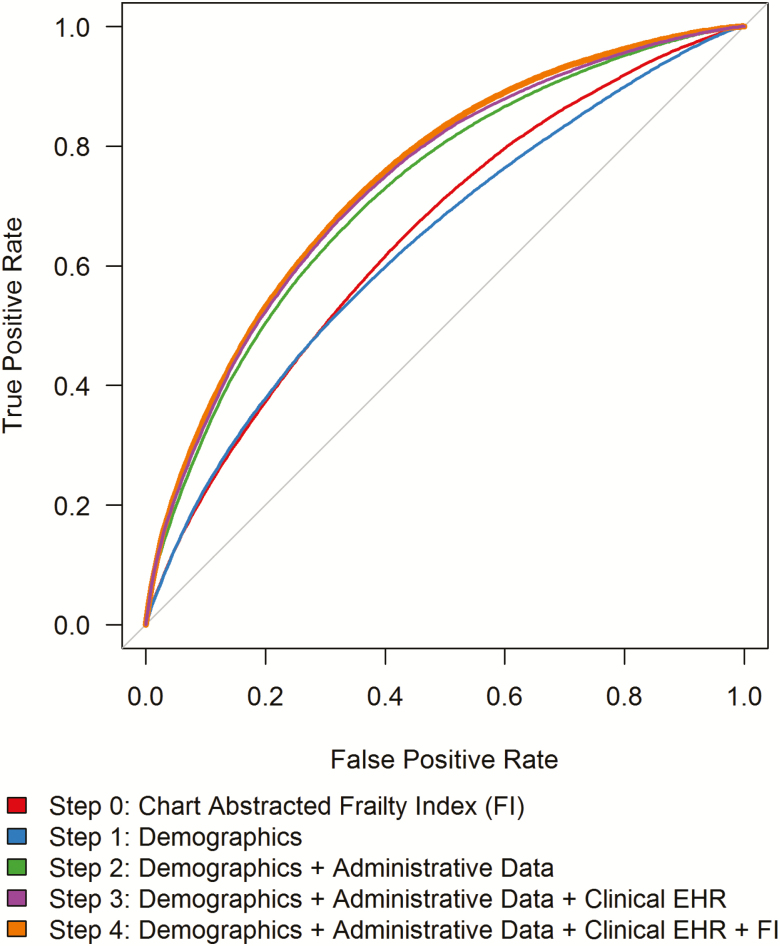
Methods: We conducted a retrospective cohort study in a single Veterans Health Administration (VHA) healthcare system of 500 hospitalizations-the majority due to heart failure-of Veterans who received regular VHA care and initiated type 2 diabetes treatment from 2001 to 2008. We measured frailty using a modified frailty index (FI, >0.21 frail). We obtained antidiabetic medication regimen and time-to-death from administrative sources. We compared FI among patients on different antidiabetic regimens. Stepwise Cox proportional hazards regression estimated time-to-death by demographic, administrative, clinical EHR, and FI data.
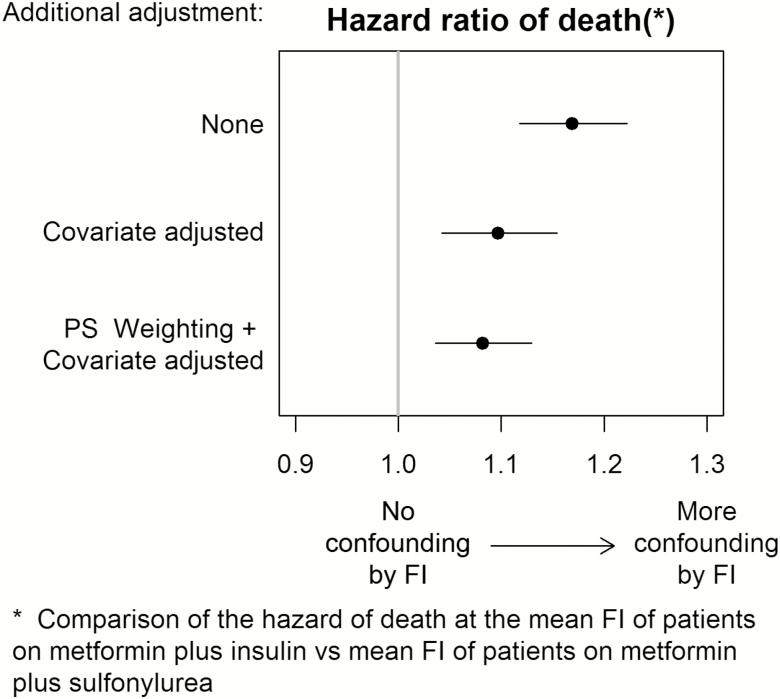
Results: Median FI was 0.22 (interquartile range 0.18, 0.27). Frailty differed across antidiabetic regimens (p < .001). An FI increase of 0.05 was associated with an increased risk of death (hazard ratio 1.45, 95% confidence interval 1.32, 1.60). Cox proportional hazards model for time-to-death including demographic, administrative, and clinical EHR data had a c-statistic of 0.70; adding FI showed marginal improvement (c-statistic 0.72).
Conclusions: Frailty was associated with antidiabetic regimen and death, and may confound that relationship. Demographic, administrative, and clinical EHR data, commonly used to balance differences among exposure groups, performed moderately well in assessing risk of death, with minimal gain from adding frailty. Study design and analytic techniques can help minimize potential confounding by frailty in observational studies.
Keywords: Diabetes; Drug-related; Epidemiology; Frailty.
Published by Oxford University Press on behalf of The Gerontological Society of America 2018.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
