

Landscape of Acquired Resistance to Osimertinib in EGFR-Mutant NSCLC and Clinical Validation of Combined EGFR and RET Inhibition with Osimertinib and BLU-667 for Acquired RET Fusion
- PMID: 30257958
- PMCID: PMC6279502
- DOI: 10.1158/2159-8290.CD-18-1022
Landscape of Acquired Resistance to Osimertinib in EGFR-Mutant NSCLC and Clinical Validation of Combined EGFR and RET Inhibition with Osimertinib and BLU-667 for Acquired RET Fusion
Abstract
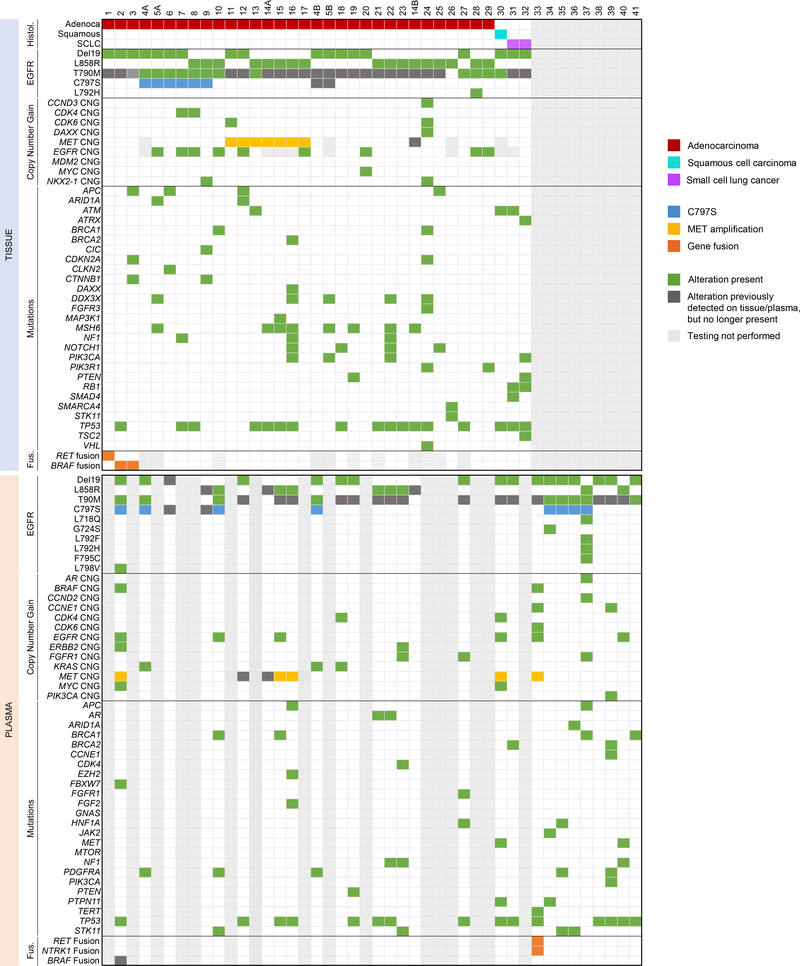
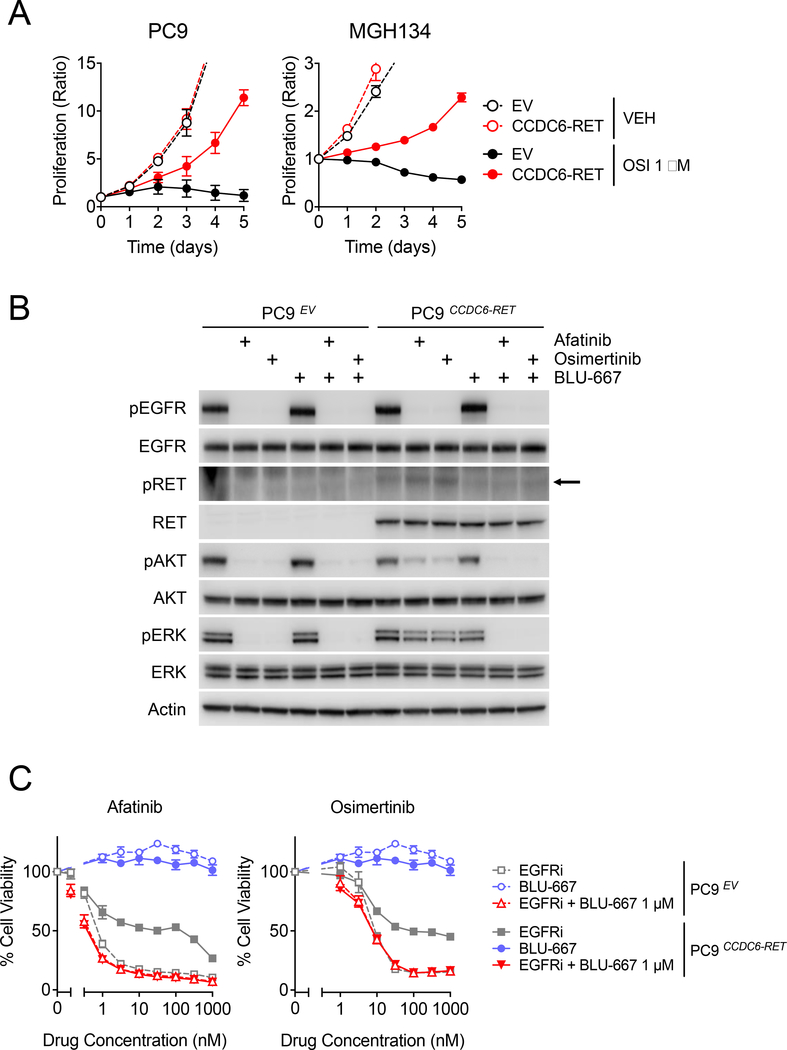
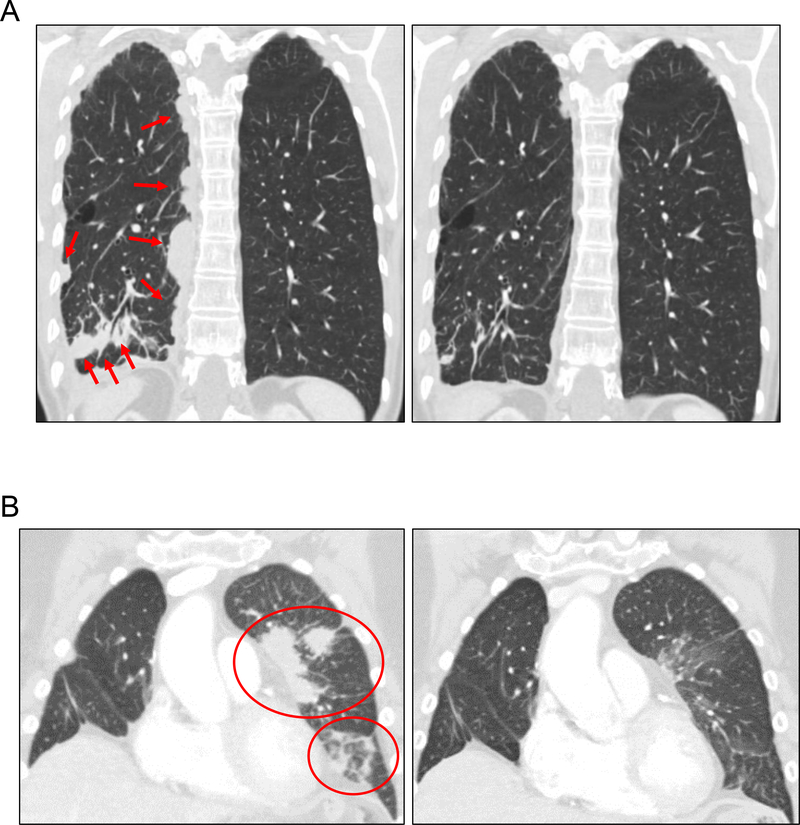
We present a cohort of 41 patients with osimertinib resistance biopsies, including 2 with an acquired CCDC6-RET fusion. Although RET fusions have been identified in resistant EGFR-mutant non-small cell lung cancer (NSCLC), their role in acquired resistance to EGFR inhibitors is not well described. To assess the biological implications of RET fusions in an EGFR-mutant cancer, we expressed CCDC6-RET in PC9 (EGFR del19) and MGH134 (EGFR L858R/T790M) cells and found that CCDC6-RET was sufficient to confer resistance to EGFR tyrosine kinase inhibitors (TKI). The selective RET inhibitors BLU-667 and cabozantinib resensitized CCDC6-RET-expressing cells to EGFR inhibition. Finally, we treated 2 patients with EGFR-mutant NSCLC and RET-mediated resistance with osimertinib and BLU-667. The combination was well tolerated and led to rapid radiographic response in both patients. This study provides proof of concept that RET fusions can mediate acquired resistance to EGFR TKIs and that combined EGFR and RET inhibition with osimertinib/BLU-667 may be a well-tolerated and effective treatment strategy for such patients. SIGNIFICANCE: The role of RET fusions in resistant EGFR-mutant cancers is unknown. We report that RET fusions mediate resistance to EGFR inhibitors and demonstrate that this bypass track can be effectively targeted with a selective RET inhibitor (BLU-667) in the clinic.This article is highlighted in the In This Issue feature, p. 1494.
©2018 American Association for Cancer Research.
Conflict of interest statement
Disclosure of Potential Conflicts of Interest:
Zofia Piotrowska has served as a compensated consultant or received honoraria for AstraZeneca, Ariad/Takeda, Novartis, AbbVie and Guardant Health, and receives institutional research funding from Novartis, Takeda, Spectrum and AstraZeneca. J.F. Gainor has served as a consultant or received honoraria from Novartis, BMS, Amgen, Agios, Regeneron, Oncorus, Genentech/Roche, Pfizer, Jounce, Incyte, Theravance, Ariad/Takeda, and Array. V.W. Zhu has received honoraria from AstraZeneca, Roche-Foundation Medicine, Roche/Genentech, and Takeda, and consulting fees from TP Therapeutics. J.J. Lin has received honoraria from Chugai and Boehringer-Ingelheim. R. Nagy and R. Lanman are employees and shareholders of Guardant Health. M. Mino-Kenudson has served as a compensated consultant for Merrimack Pharmaceuticals and H3 Biomedicine. A.J. Iafrate holds equity in ArcherDX. R.S. Heist has served as a consultant for Boehringer-Ingelheim, Tarveda and Novartis and receives research funding (to institution) from Celgene, Roche, Takeda, Peregrine, Novartis, Corvus, Incyte, Debiopharm, Mirati, AbbVie, Millenium, Daichii Sankyo, Agios and Exelixis. A.T. Shaw has served as a compensated consultant or received honoraria from Pfizer, Novartis, Genentech/Roche, Ignyta, Blueprint Medicines, LOXO, Daiichi-Sankyo, Ariad/Takeda, Chugai, Taiho Pharmaceuticals, EMD Serono, KSQ Therapeutics, Foundation Medicine, Natera, Guardant, and TP Therapeutics; and serves on the scientific advisory board of Blueprint Medicines. E.K. Evans, C. Clifford and B. Wolf are employees and shareholders of Blueprint Medicines. SH.I. Ou received honoraria from Pfizer, Roche/Genentech/Ignyta, Takeda/ARIAD, AstraZeneca, Foundation Medicine and is member of the Scientific Advisory Board of TP Therapeutics and has stock ownership in TP Therapeutics. A.N. Hata reports research funding from Novartis, Amgen and Relay therapeutics. LVS declares advisory relationships, honoraria or research funding from AstraZeneca, Blueprint Medicines, Novartis, Pfizer, Genentech, Boehringer Ingelheim, and Merrimack Pharmaceuticals. No potential conflicts of interest were disclosed by the other authors.
Figures
References
-
- Soria JC, Ohe Y, Vansteenkiste J, et al. Osimertinib in Untreated EGFR-Mutated Advanced Non-Small-Cell Lung Cancer. N Engl J Med. 2018;378(2):113–125. - PubMed
-
- Piotrowska Z, Thress K, Mooradian MJ, et al. MET amplification (amp) is a mjaor resistance mechanism to osimertinib. Paper presented at: Annual Meeting of the American Society of Clinical Oncology2017; Chicago, IL.
-
- Zhang Q, Zhang XC, Yang JJ, et al. EGFR L792H and G796R: Two Novel Mutations Mediating Resistance to the Third-Generation EGFR Tyrosine Kinase Inhibitor Osimertinib. J Thorac Oncol. 2018;13(9):1415–1421. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
