

Multiple Endocrine Neoplasia Type 1: A Case Report With Review of Imaging Findings
- PMID: 30258300
- PMCID: PMC6135292
- DOI: 10.31486/toj.17.0019
Multiple Endocrine Neoplasia Type 1: A Case Report With Review of Imaging Findings
Abstract
Background: Multiple endocrine neoplasia type 1 (MEN1) is a rare, autosomal dominant inherited syndrome caused by mutations in the MEN1 tumor suppressor gene. The diagnosis is defined clinically by the presence of 2 or more primary MEN1 tumors (parathyroid, anterior pituitary, and pancreatic islet). We describe the case of a patient who presented with classic history and imaging findings for MEN1.
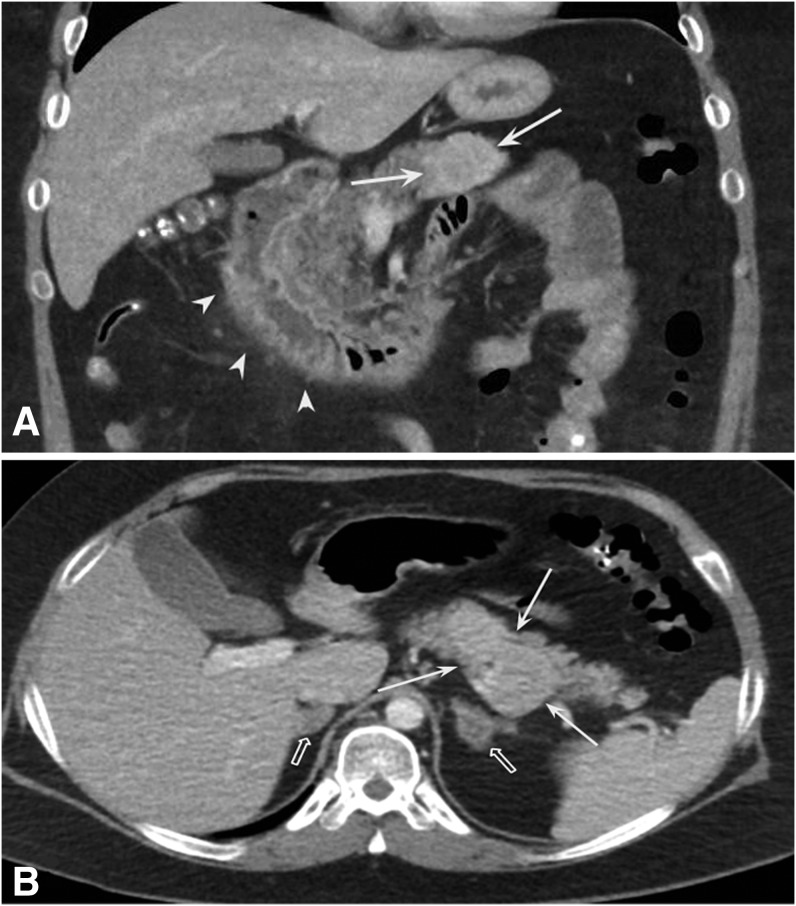
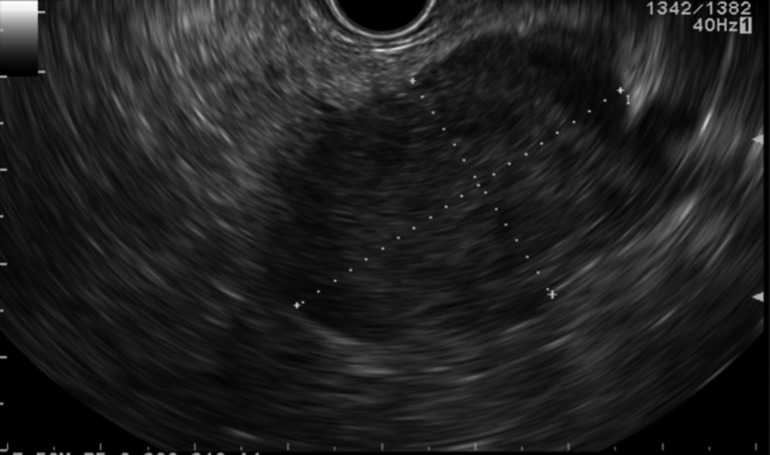
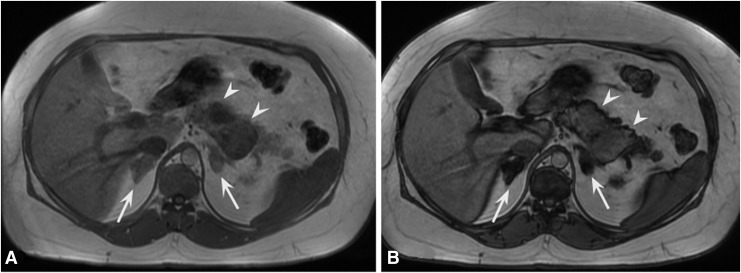
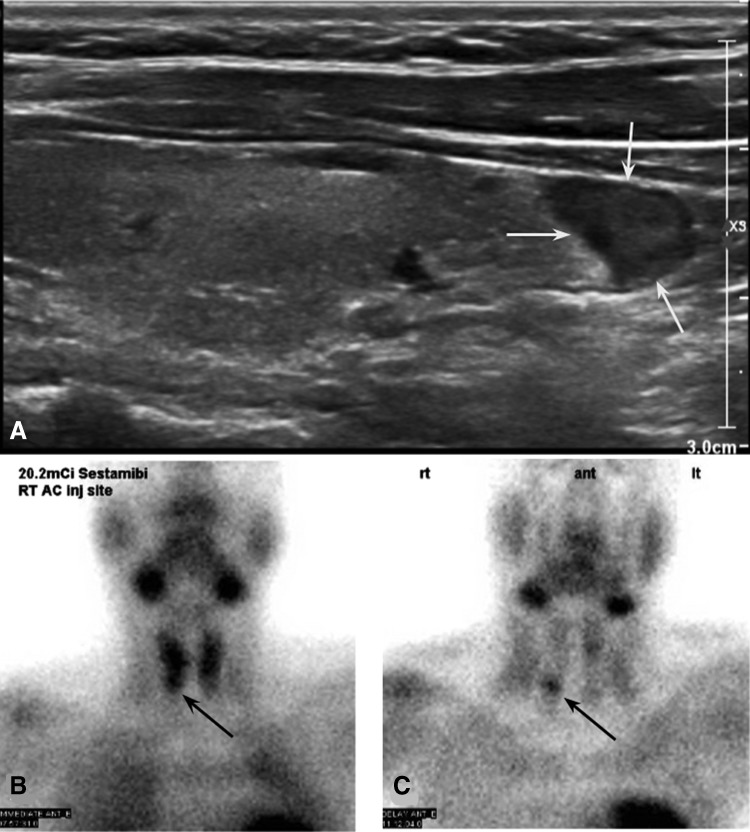
Case report: A male in his early thirties with a history of hyperparathyroidism and a transsphenoidal prolactinoma resection presented years later with abdominal symptoms concerning for Zollinger-Ellison syndrome: worsening epigastric abdominal pain, nausea, vomiting, and diarrhea. Contrast-enhanced computed tomography (CT) of the abdomen revealed hyperenhancing pancreatic lesions and duodenal inflammation, suggesting pancreatic neuroendocrine tumor (gastrinoma) with secondary duodenitis. Bilateral indeterminate hypoattenuating adrenal nodules were also seen on contrast-enhanced CT, and follow-up magnetic resonance imaging confirmed benign adrenal adenomas. Furthermore, thyroid ultrasound and sestamibi scintigraphy revealed a parathyroid adenoma. With confirmatory imaging findings, history, and presenting symptoms, the patient was clinically diagnosed with MEN1 syndrome and underwent surgical and medical management.
Conclusion: This case exhibits the classic history with corresponding imaging findings of MEN1 syndrome, including pancreatic neuroendocrine tumors, parathyroid adenoma, and adrenal adenomas. High clinical suspicion for MEN1 should lead to endocrinology evaluation with appropriate laboratory workup and targeted imaging evaluation of the typical endocrine organs as described for this patient.
Keywords: Adrenal gland neoplasms; Zollinger-Ellison syndrome; gastrinoma; multiple endocrine neoplasia type 1; neuroendocrine tumors; parathyroid neoplasms; pituitary neoplasms.
Figures
References
-
- Ito T, Igarashi H, Uehara H, Berna MJ, Jensen RT. Causes of death and prognostic factors in multiple endocrine neoplasia type 1: a prospective study: comparison of 106 MEN1/Zollinger-Ellison syndrome patients with 1613 literature MEN1 patients with or without pancreatic endocrine tumors. Medicine (Baltimore). 2013. May;92(3):135-181. doi: 10.1097/MD.0b013e3182954af1. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources