

Quantitative Assessment of the Anatomical Footprint of the C1 Pedicle Relative to the Lateral Mass: A Guide for C1 Lateral Mass Fixation
- PMID: 30258757
- PMCID: PMC6149043
- DOI: 10.1177/2192568217744530
Quantitative Assessment of the Anatomical Footprint of the C1 Pedicle Relative to the Lateral Mass: A Guide for C1 Lateral Mass Fixation
Abstract
Study design: Anatomic study.
Objectives: To determine the relationship of the anatomical footprint of the C1 pedicle relative to the lateral mass (LM).
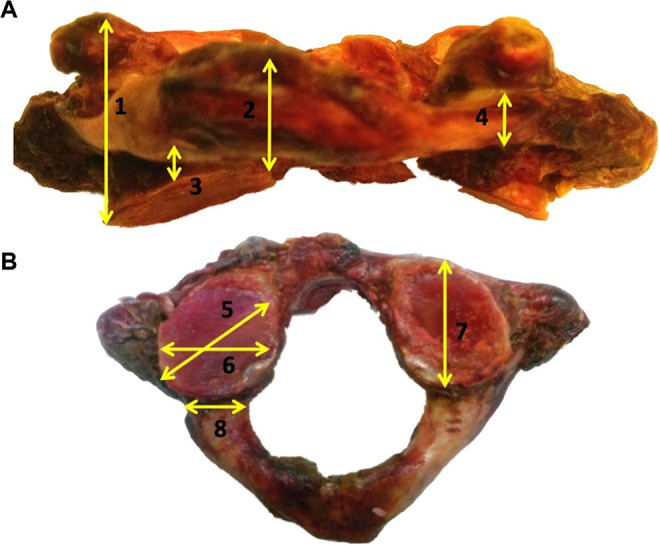
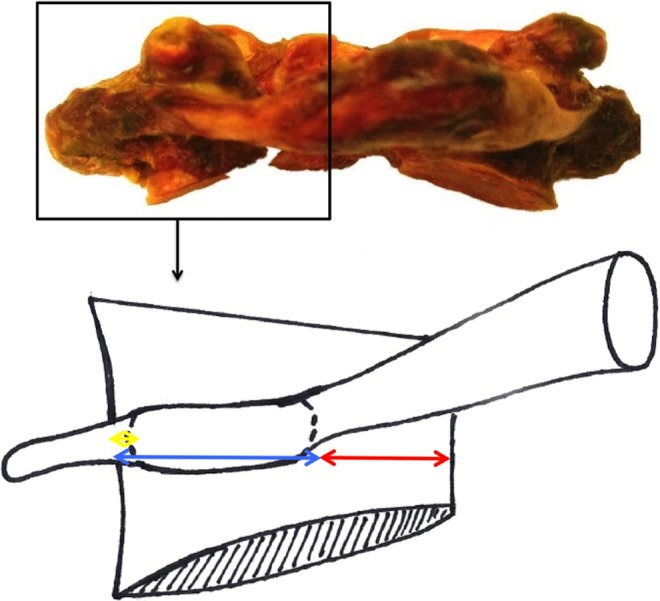
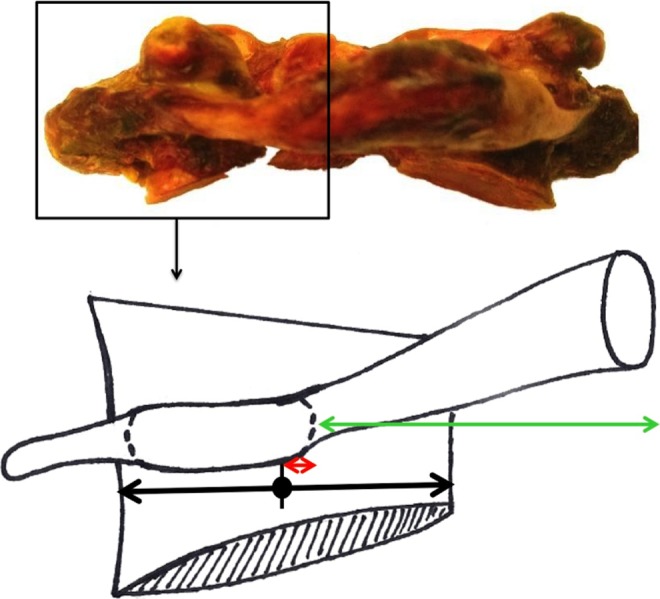
Methods: Anatomic measurements were made on fresh frozen human cadaveric C1 specimens: pedicle width/height, LM width/height (minimum/maximum), LM depth, distance between LM's medial aspect and pedicle's medial border, distance between LM's lateral aspect to pedicle's lateral border, distance between pedicle's inferior aspect and LM's inferior border, distance between arch's midline and pedicle's medial border. The percentage of LM medial to the pedicle and the distance from the center of the LM to the pedicle's medial wall were calculated.
Results: A total of 42 LM were analyzed. The C1 pedicle's lateral aspect was nearly confluent with the LM's lateral border. Average pedicle width was 9.0 ± 1.1 mm, and average pedicle height was 5.0 ± 1.1 mm. Average LM width and depth were 17.0 ± 1.6 and 17.2 ± 1.6 mm, respectively. There was 6.9 ± 1.5 mm of bone medial to the medial C1 pedicle, which constituted 41% ± 9% of the LM's width. The distance from C1 arch's midline to the medial pedicle was 13.5 ± 2.0 mm. The LM's center was 1.6 ± 1 mm lateral to the medial pedicle wall. There was on average 3.5 ± 0.6 mm of the LM inferior to the pedicle inferior border.
Conclusions: The center of the lateral mass is 1.6 ± 1 mm lateral to the medial wall of the C1 pedicle and approximately 15 mm from the midline. There is 6.9 ± 1.5 mm of bone medial to the medial C1 pedicle. Thus, the medial aspect of C1 pedicle may be used as an anatomic reference for locating the center of the C1 LM for screw fixation.
Keywords: C1; atlas; lateral mass; pedicle; upper cervical spine.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Similar articles
-
[Anatomic identification of the location of the pedicle of atlas with the lateral mass of C2 to C4 as the landmark].Zhonghua Wai Ke Za Zhi. 2005 Jun 15;43(12):774-6. Zhonghua Wai Ke Za Zhi. 2005. PMID: 16083577 Chinese.
-
Posterior screw placement on the lateral mass of atlas: an anatomic study.Spine (Phila Pa 1976). 2004 Mar 1;29(5):500-3. doi: 10.1097/01.brs.0000113874.82587.33. Spine (Phila Pa 1976). 2004. PMID: 15129062
-
Anatomic considerations for the pedicle screw placement in the first cervical vertebra.Spine (Phila Pa 1976). 2005 Jul 1;30(13):1519-23. doi: 10.1097/01.brs.0000168546.17788.49. Spine (Phila Pa 1976). 2005. PMID: 15990666 Clinical Trial.
-
[ANATOMIC STUDY ON ENTRY POINT AND IMPLANT TECHNIQUE FOR C2 PEDICLE SCREW FIXATION].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2015 Feb;29(2):175-8. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2015. PMID: 26455145 Chinese.
-
Liliequist membrane: A systematic review of history, anatomy, clinical importance, and surgical challenges.Clin Neurol Neurosurg. 2024 Jul;242:108322. doi: 10.1016/j.clineuro.2024.108322. Epub 2024 May 11. Clin Neurol Neurosurg. 2024. PMID: 38795689
Cited by
-
The Intersection Between Lateral Mass and Inferomedial Edge of the C1 Posterior Arch: A Reference Point for C1 Lateral Mass Screw Insertion.Neurospine. 2021 Jun;18(2):328-335. doi: 10.14245/ns.2040814.407. Epub 2021 Jun 30. Neurospine. 2021. PMID: 34218613 Free PMC article.
-
Exploring the prevalence and impact on craniocervical spine surgery of ponticulus posticus on atlas lamina thickness.J Craniovertebr Junction Spine. 2025 Apr-Jun;16(2):195-199. doi: 10.4103/jcvjs.jcvjs_53_25. Epub 2025 Jul 3. J Craniovertebr Junction Spine. 2025. PMID: 40756487 Free PMC article.
References
-
- Brooks AL, Jenkins EB. Atlanto-axial arthrodesis by the wedge compression method. J Bone Joint Surg Am. 1978;60:279–284. - PubMed
-
- Gallie WE. Fractures and dislocations of cervical spine. Am J Surg. 1939;46:495–499.
-
- Holness R, Huestis W, Howes W, Langille R. Posterior stabilization with an interlaminar clamp in cervical injuries: technical note and review of the long term experience with the method. Neurosurgery. 1984;14:318–322. - PubMed
-
- Jeanneret B, Magerl F. Primary posterior fusion C1/2 in odontoid fractures: indications, technique, and results of transarticular screw fixation. J Spinal Disord. 1992;5:464–475. doi:10.1097/00002517-199212000-00012. - PubMed
-
- Du J, Aichmair A, Kueper J, Wright T, Lebl D. Biomechanical analysis of screw constructs for atlantoaxial fixation in cadavers: a systematic review and meta-analysis. J Neurosurg Spine. 2015;22:151–161. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
