

Rituximab-induced hypogammaglobulinemia in patients with neuromyelitis optica spectrum disorders
- PMID: 30258855
- PMCID: PMC6148550
- DOI: 10.1212/NXI.0000000000000498
Rituximab-induced hypogammaglobulinemia in patients with neuromyelitis optica spectrum disorders
Abstract
Objective: To evaluate the long-term effects of rituximab (RTX) on total and specific immunoglobulins (Igs) in patients with neuromyelitis optica spectrum disorders (NMOSDs).
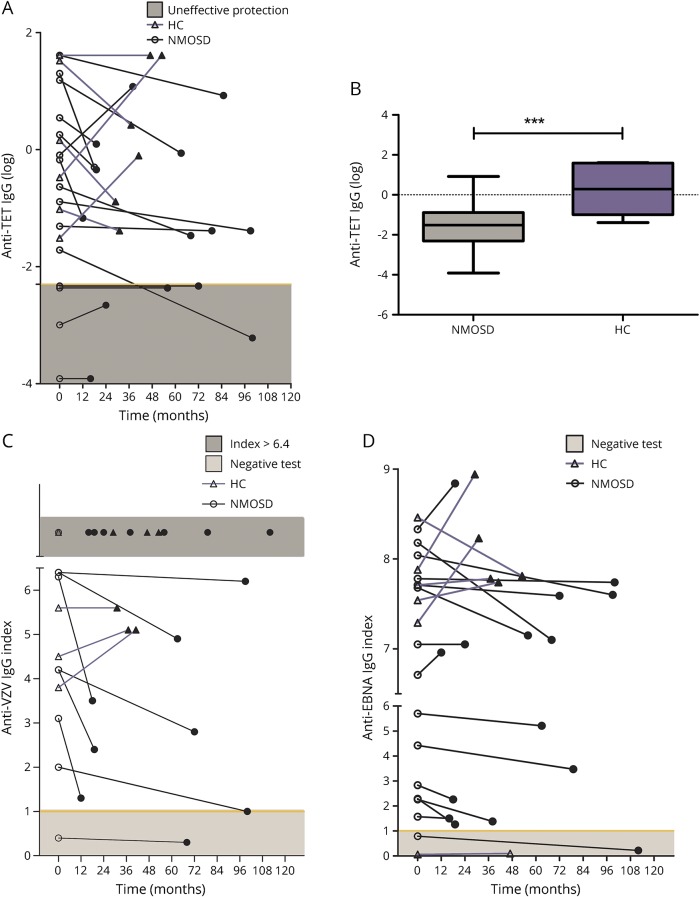
Methods: Total IgG, IgA, and IgM levels were evaluated in 15 patients with NMOSDs treated with RTX (median follow-up 70 months). Anti-aquaporin 4 (AQP4)-IgG titration was performed on samples from 9 positive patients. Anti-tetanus (TET), anti-varicella-zoster virus (VZV), and anti-Epstein-Barr virus nuclear antigen (EBNA) IgGs were also tested in patients with NMOSDs and in 6 healthy controls (HCs).
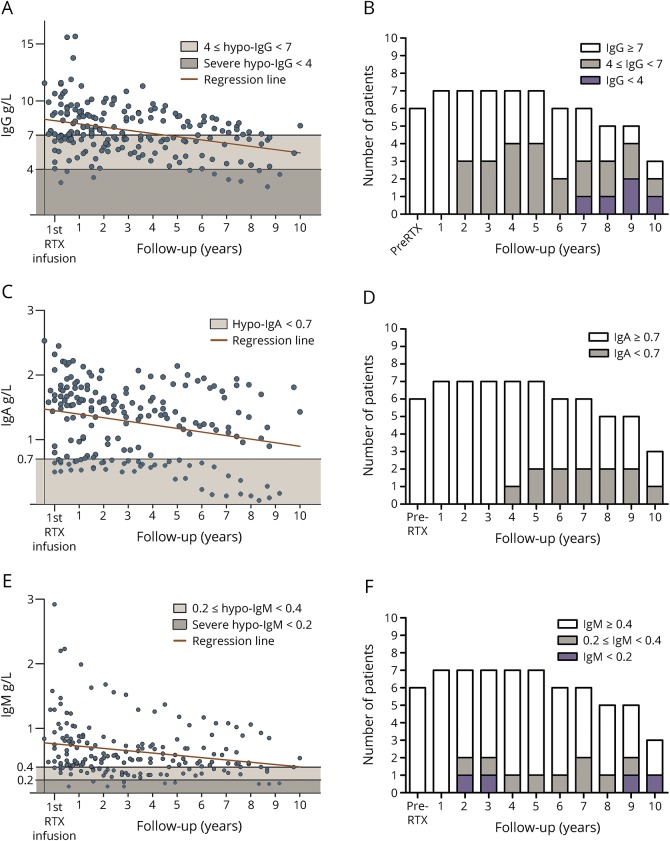
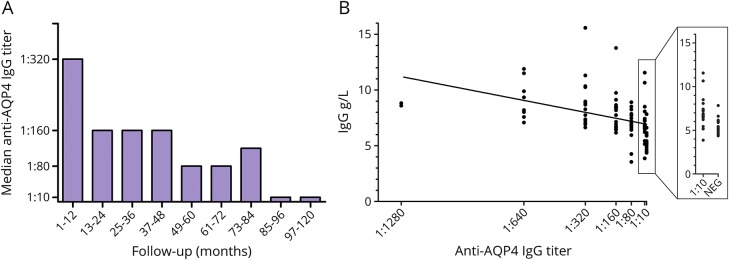
Results: RTX reduced total IgG by 0.42 g/L per year, IgA by 0.08 g/L per year, and IgM by 0.07 g/L per year. Hypogammaglobulinemia (hypo-IgG) (IgG < 7 g/L) developed in 11/15 patients. Severe hypo-IgG (IgG < 4 g/L) was found in 3/15 patients, of whom 2 patients developed serious infectious complications. In group analysis, anti-AQP4 IgG titers were reduced by RTX over time, and a significant correlation between anti-AQP4 IgG titers and total IgG levels was found. The effects of RTX were observed on pathogen-specific IgGs as well. In particular, the levels of anti-TET IgG in patients were significantly lower than those in HCs. The half-life of anti-TET IgG was reduced by about 50% in patients compared with the general population.
Conclusions: Long-term RTX treatment is associated with the risk of hypo-Ig and reduction of anti-TET protection in patients with NMOSDs. Results obtained in this study suggest the importance of monitoring total and specific Ig levels before and during treatment with anti-CD20 drugs to prevent hypo-Ig-related complications and to optimize clinical management.
Figures
Similar articles
-
Rituximab-Induced Hypogammaglobulinemia and Risk of Infection in Neuromyelitis Optica Spectrum Disorders: A 14-Year Real-Life Experience.Neurol Neuroimmunol Neuroinflamm. 2022 Jul 19;9(5):e1179. doi: 10.1212/NXI.0000000000001179. Print 2022 Sep. Neurol Neuroimmunol Neuroinflamm. 2022. PMID: 35853752 Free PMC article.
-
Impact of rituximab on immunoglobulin concentrations and B cell numbers after cyclophosphamide treatment in patients with ANCA-associated vasculitides.PLoS One. 2012;7(5):e37626. doi: 10.1371/journal.pone.0037626. Epub 2012 May 21. PLoS One. 2012. PMID: 22629432 Free PMC article.
-
Aquaporin-4 antibody titration in NMO patients treated with rituximab: A retrospective study.Neurol Neuroimmunol Neuroinflamm. 2016 Dec 15;4(2):e317. doi: 10.1212/NXI.0000000000000317. eCollection 2017 Mar. Neurol Neuroimmunol Neuroinflamm. 2016. PMID: 28054001 Free PMC article.
-
Evaluation of effect of empirical attack-preventive immunotherapies in neuromyelitis optica spectrum disorders: An update systematic review and meta -analysis.J Neuroimmunol. 2022 Feb 15;363:577790. doi: 10.1016/j.jneuroim.2021.577790. Epub 2021 Dec 16. J Neuroimmunol. 2022. PMID: 34959021
-
AQP4-IgG-seropositive neuromyelitis optica spectrum disorder (NMOSD) coexisting with anti-N-methyl-D-aspartate receptor (NMDAR) encephalitis: A case report and literature review.Mult Scler Relat Disord. 2019 Oct;35:185-192. doi: 10.1016/j.msard.2019.07.008. Epub 2019 Jul 20. Mult Scler Relat Disord. 2019. PMID: 31398657 Review.
Cited by
-
Re-Evaluating the Use of IFN-β and Relapsing Multiple Sclerosis: Safety, Efficacy and Place in Therapy.Degener Neurol Neuromuscul Dis. 2020 Jun 26;10:29-38. doi: 10.2147/DNND.S224912. eCollection 2020. Degener Neurol Neuromuscul Dis. 2020. PMID: 32617031 Free PMC article. Review.
-
Long-term tolerability, safety and efficacy of rituximab in neuromyelitis optica spectrum disorder: a prospective study.J Neurol. 2019 Mar;266(3):642-650. doi: 10.1007/s00415-019-09180-9. Epub 2019 Jan 11. J Neurol. 2019. PMID: 30635724
-
Multiple Sclerosis, COVID-19 and Vaccines: Making the Point.Neurol Ther. 2021 Dec;10(2):627-649. doi: 10.1007/s40120-021-00288-7. Epub 2021 Oct 8. Neurol Ther. 2021. PMID: 34625925 Free PMC article. Review.
-
Effects of the COVID-19 Pandemic on Patients With NMO Spectrum Disorders and MOG-Antibody-Associated Diseases: COPANMO(G)-Study.Neurol Neuroimmunol Neuroinflamm. 2023 Jan 24;10(2):e200082. doi: 10.1212/NXI.0000000000200082. Print 2023 Mar. Neurol Neuroimmunol Neuroinflamm. 2023. PMID: 36693760 Free PMC article.
-
Update on neuromyelitis optica spectrum disorder.Curr Opin Ophthalmol. 2020 Nov;31(6):462-468. doi: 10.1097/ICU.0000000000000703. Curr Opin Ophthalmol. 2020. PMID: 33009077 Free PMC article. Review.
References
-
- Smolewski P, Robak T. The preclinical discovery of rituximab for the treatment of non-Hodgkin's lymphoma. Expert Opin Drug Discov 2015;10:791–808. - PubMed
-
- Seyfizadeh N, Seyfizadeh N, Hasenkamp J, Huerta-Yepez S. A molecular perspective on rituximab: a monoclonal antibody for B cell non Hodgkin lymphoma and other affections. Crit Rev Oncol Hematol 2016;97:275–290. - PubMed
-
- Maloney DG, Grillo-lo AJ, White CA, et al. . IDEC-C2B8 (rituximab) anti-CD20 monoclonal antibody therapy in patients with relapsed low-Grade non-Hodgkin's lymphoma. Blood 1997;90:2188–2195. - PubMed
-
- Edwards JCW, Szczepański L, Szechiński J, et al. . Efficacy of B-Cell–Targeted therapy with rituximab in patients with rheumatoid arthritis. N Engl J Med 2004;350:2572–2581. - PubMed
-
- Edwards JC, Cambridge G. Sustained improvement in rheumatoid arthritis following a protocol designed to deplete B lymphocytes. Rheumatology (Oxford) 2001;40:205–211. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous