

Atrial fibrillation and chronic kidney disease: A review of options for therapeutic anticoagulation to reduce thromboembolism risk
- PMID: 30259531
- PMCID: PMC6489944
- DOI: 10.1002/clc.23085
Atrial fibrillation and chronic kidney disease: A review of options for therapeutic anticoagulation to reduce thromboembolism risk
Abstract
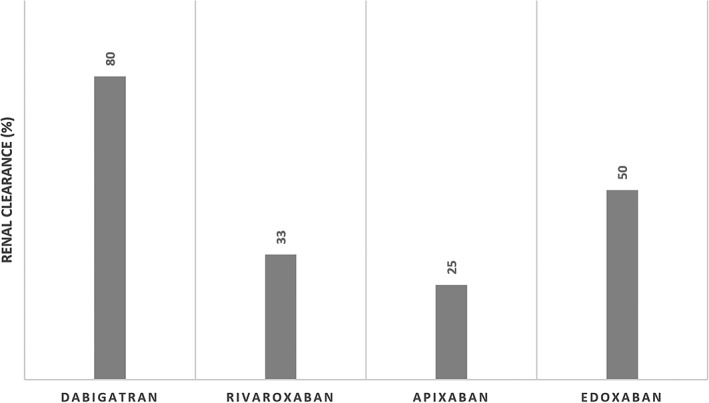
Atrial fibrillation and chronic kidney disease (CKD) commonly occur together, which poses a therapeutic dilemma due to increased risk of both systemic thromboembolism and bleeding. Chronic kidney disease also has implications for medication selection. The objective of this review is to evaluate the options for anticoagulation for thromboembolism prevention in patients with atrial fibrillation and chronic kidney disease. We searched PubMed for studies of patients with atrial fibrillation and CKD on warfarin or a direct oral anticoagulant (DOAC) for thromboembolism prevention through January 1 2018, in addition to evaluating major trials evaluating DOACs and warfarin use as well as society guidelines. For patients with mild to moderate chronic kidney disease, primarily observational data supports the use of warfarin, and high quality trial data and meta-analyses support the use and possible superiority of DOACs. For patients with severe chronic kidney disease, there are limited data on warfarin which supports its use, and data for DOACs is limited primarily to pharmacologic studies which support dose reductions but lack information on patient outcomes. For patients with end-stage renal disease, studies on warfarin are conflicting, but the majority suggest a lack of benefit and possible harm; studies in DOACs are very limited, but apixaban is the least renally cleared and may be both safe and effective. In conclusion, warfarin or DOACs may be used based on the degree of severity of chronic kidney disease, but further study in needed in patients with end-stage renal disease.
Keywords: arrhythmia/all; atrial fibrillation; general clinical cardiology/adult; kidney disease; pharmacology; stroke prevention.
© 2018 Wiley Periodicals, Inc.
Figures
Similar articles
-
Efficacy and safety of direct oral anticoagulants in patients with atrial fibrillation and chronic kidney disease.Pacing Clin Electrophysiol. 2019 Nov;42(11):1463-1470. doi: 10.1111/pace.13811. Epub 2019 Oct 16. Pacing Clin Electrophysiol. 2019. PMID: 31599969
-
Nonvitamin K-dependent oral anticoagulants (NOACs) in chronic kidney disease patients with atrial fibrillation.Thromb Res. 2017 Jul;155:38-47. doi: 10.1016/j.thromres.2017.04.027. Epub 2017 May 4. Thromb Res. 2017. PMID: 28482261 Review.
-
A systematic review of direct oral anticoagulant use in chronic kidney disease and dialysis patients with atrial fibrillation.Nephrol Dial Transplant. 2019 Feb 1;34(2):265-277. doi: 10.1093/ndt/gfy031. Nephrol Dial Transplant. 2019. PMID: 29509922
-
A Review of Direct Oral Anticoagulants in Patients With Stage 5 or End-Stage Kidney Disease.Ann Pharmacother. 2022 Jun;56(6):691-703. doi: 10.1177/10600280211040093. Epub 2021 Aug 29. Ann Pharmacother. 2022. PMID: 34459281 Review.
-
[Non vitamin-K dependent oral anticoagulants (NOACs) in chronic kidney disease patients with non-valvular atrial fibrillation].G Ital Nefrol. 2017 Apr;34(2):58-73. G Ital Nefrol. 2017. PMID: 28682563 Review. Italian.
Cited by
-
Risks of anticoagulation in patients with chronic kidney disease and atrial fibrillation: More than just bleeding?Res Pract Thromb Haemost. 2019 Mar 5;3(2):147-148. doi: 10.1002/rth2.12188. eCollection 2019 Apr. Res Pract Thromb Haemost. 2019. PMID: 31011695 Free PMC article. No abstract available.
-
Therapeutic anticoagulation complications in the elderly: a case report.BMC Geriatr. 2022 Feb 5;22(1):102. doi: 10.1186/s12877-022-02781-6. BMC Geriatr. 2022. PMID: 35123396 Free PMC article.
-
Atrial fibrillation and kidney disease: insights on a close relationship.Intern Emerg Med. 2019 Oct;14(7):1025-1027. doi: 10.1007/s11739-019-02141-0. Epub 2019 Jul 17. Intern Emerg Med. 2019. PMID: 31317312 No abstract available.
-
Management dilemmas in restarting anticoagulation after gastrointestinal bleeding.Proc (Bayl Univ Med Cent). 2022 Mar 9;35(3):322-327. doi: 10.1080/08998280.2022.2043707. eCollection 2022. Proc (Bayl Univ Med Cent). 2022. PMID: 35518826 Free PMC article.
-
Association of atrial fibrillation and clinical outcomes in adults with chronic kidney disease: A propensity score-matched analysis.PLoS One. 2020 Mar 18;15(3):e0230189. doi: 10.1371/journal.pone.0230189. eCollection 2020. PLoS One. 2020. PMID: 32187219 Free PMC article.
References
-
- Mitsuma W, Matsubara T, Hatada K, et al. Clinical characteristics of hemodialysis patients with atrial fibrillation: the RAKUEN (registry of atrial fibrillation in chronic kidney disease under hemodialysis from Niigata) study. J Cardiol. 2016;68(2):148‐155. 10.1016/j.jjcc.2015.08.023. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
