

Propofol for Treatment-Resistant Depression: A Pilot Study
- PMID: 30260415
- PMCID: PMC6276046
- DOI: 10.1093/ijnp/pyy085
Propofol for Treatment-Resistant Depression: A Pilot Study
Abstract
Background: We hypothesized that propofol, a unique general anesthetic that engages N-methyl-D-aspartate and gamma-aminobutyric acid receptors, has antidepressant properties. This open-label trial was designed to collect preliminary data regarding the feasibility, tolerability, and efficacy of deep propofol anesthesia for treatment-resistant depression.
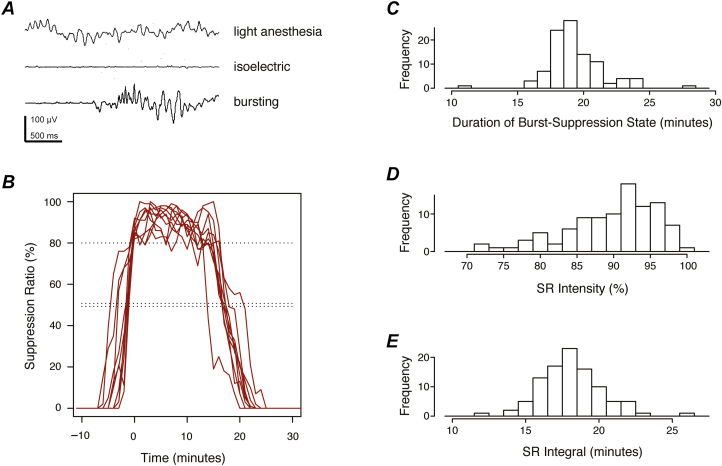
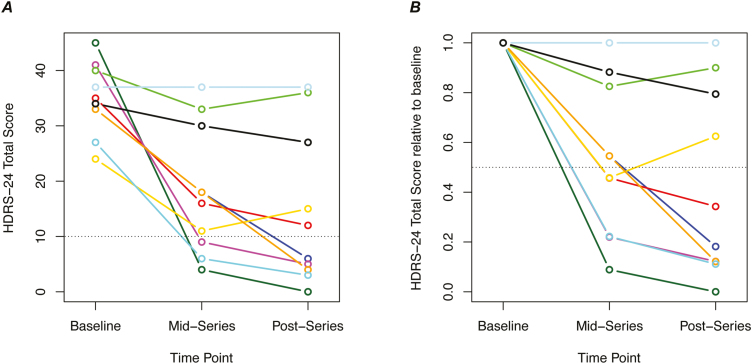
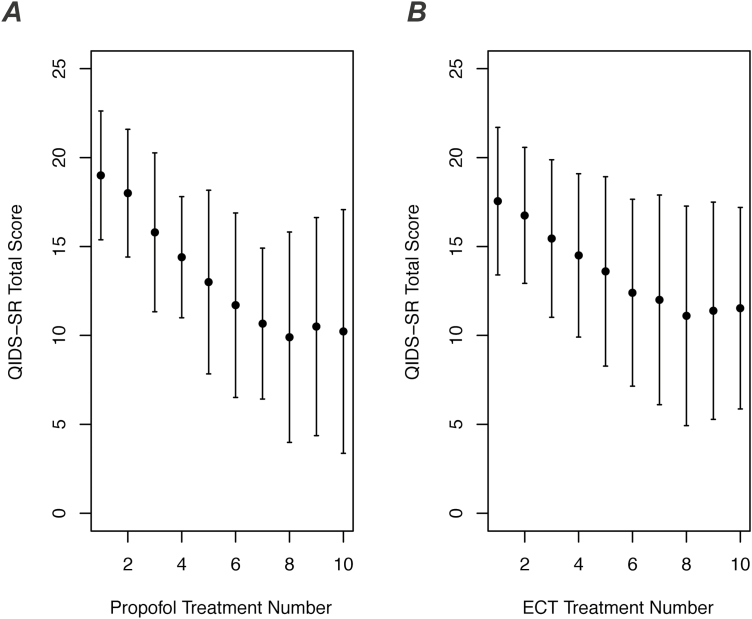
Methods: Ten participants with moderate-to-severe medication-resistant depression (age 18-45 years and otherwise healthy) each received a series of 10 propofol infusions. Propofol was dosed to strongly suppress electroencephalographic activity for 15 minutes. The primary depression outcome was the 24-item Hamilton Depression Rating Scale. Self-rated depression scores were compared with a group of 20 patients who received electroconvulsive therapy.
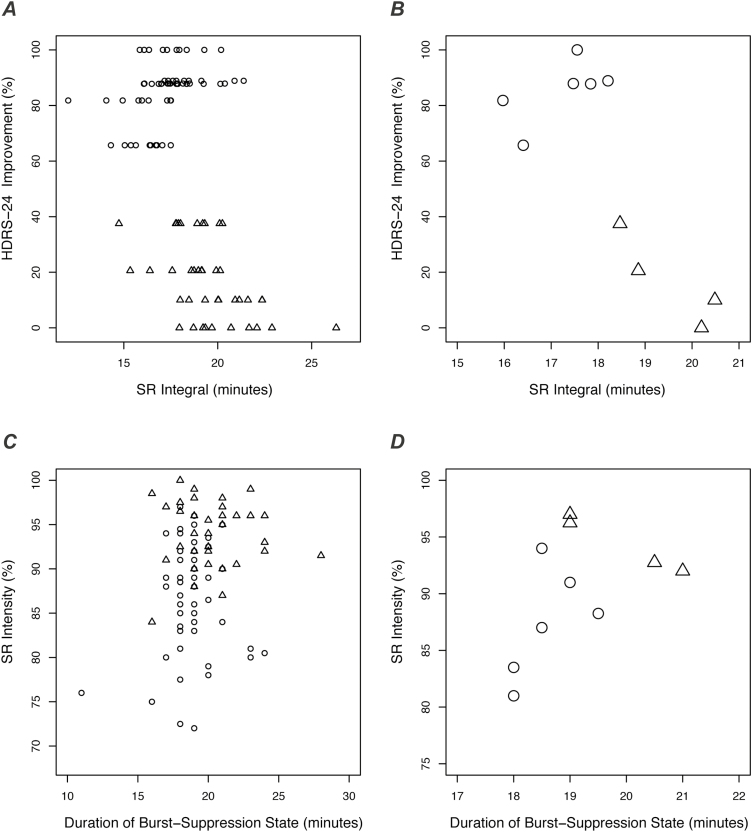
Results: Propofol treatments were well tolerated by all subjects. No serious adverse events occurred. Montreal Cognitive Assessment scores remained stable. Hamilton scores decreased by a mean of 20 points (range 0-45 points), corresponding to a mean 58% improvement from baseline (range 0-100%). Six of the 10 subjects met the criteria for response (>50% improvement). Self-rated depression improved similarly in the propofol group and electroconvulsive therapy group. Five of the 6 propofol responders remained well for at least 3 months. In posthoc analyses, electroencephalographic measures predicted clinical response to propofol.
Conclusions: These findings demonstrate that high-dose propofol treatment is feasible and well tolerated by individuals with treatment-resistant depression who are otherwise healthy. Propofol may trigger rapid, durable antidepressant effects similar to electroconvulsive therapy but with fewer side effects. Controlled studies are warranted to further evaluate propofol's antidepressant efficacy and mechanisms of action. ClinicalTrials.gov: NCT02935647.
Figures
References
-
- Berman RM, Cappiello A, Anand A, Oren DA, Heninger GR, Charney DS, Krystal JH(2000)Antidepressant effects of ketamine in depressed patients. Biol Psychiatry 47:351–354. - PubMed
-
- Carl C, Engelhardt W, Teichmann G, Fuchs G(1988)Open comparative study with treatment-refractory depressed patients: electroconvulsive therapy–anesthetic therapy with isoflurane (preliminary report). Pharmacopsychiatry 21:432–433. - PubMed
-
- Coyle CM, Laws KR(2015)The use of ketamine as an antidepressant: a systematic review and meta-analysis. Hum Psychopharmacol 30:152–163. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
