

Ageing, Cellular Senescence and Neurodegenerative Disease
- PMID: 30261683
- PMCID: PMC6213570
- DOI: 10.3390/ijms19102937
Ageing, Cellular Senescence and Neurodegenerative Disease
Abstract
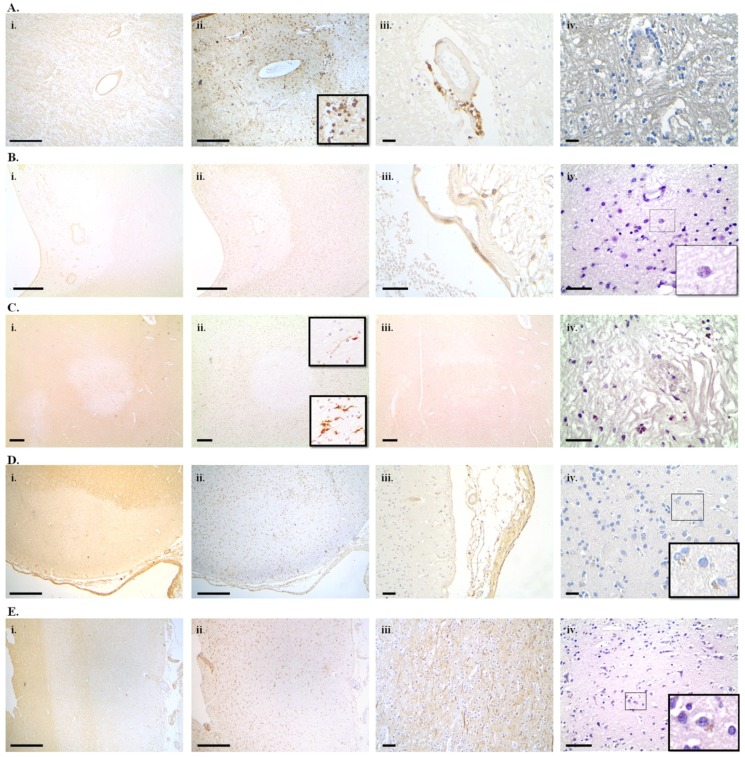
Ageing is a major risk factor for developing many neurodegenerative diseases. Cellular senescence is a homeostatic biological process that has a key role in driving ageing. There is evidence that senescent cells accumulate in the nervous system with ageing and neurodegenerative disease and may predispose a person to the appearance of a neurodegenerative condition or may aggravate its course. Research into senescence has long been hindered by its variable and cell-type specific features and the lack of a universal marker to unequivocally detect senescent cells. Recent advances in senescence markers and genetically modified animal models have boosted our knowledge on the role of cellular senescence in ageing and age-related disease. The aim now is to fully elucidate its role in neurodegeneration in order to efficiently and safely exploit cellular senescence as a therapeutic target. Here, we review evidence of cellular senescence in neurons and glial cells and we discuss its putative role in Alzheimer's disease, Parkinson's disease and multiple sclerosis and we provide, for the first time, evidence of senescence in neurons and glia in multiple sclerosis, using the novel GL13 lipofuscin stain as a marker of cellular senescence.
Keywords: Alzheimer’s disease; Parkinson’s disease; SenTraGorTM (GL13); ageing; cellular senescence; lipofuscin; multiple sclerosis; neurodegeneration; senolytics.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Rocca W.A., Petersen R.C., Knopman D.S., Hebert L.E., Evans D.A., Hall K.S., Gao S., Unverzagt F.W., Langa K.M., Larson E.B., et al. Trends in the incidence and prevalence of Alzheimer’s disease, dementia, and cognitive impairment in the United States. Alzheimers Dement. 2011;7:80–93. doi: 10.1016/j.jalz.2010.11.002. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
