

Discordance between 10-year cardiovascular risk estimates using the ACC/AHA 2013 estimator and coronary artery calcium in individuals from 5 racial/ethnic groups: Comparing MASALA and MESA
- PMID: 30262414
- PMCID: PMC6295226
- DOI: 10.1016/j.atherosclerosis.2018.09.015
Discordance between 10-year cardiovascular risk estimates using the ACC/AHA 2013 estimator and coronary artery calcium in individuals from 5 racial/ethnic groups: Comparing MASALA and MESA
Abstract
Background and aims: South Asian (SA) individuals are thought to represent a group that is at high-risk for atherosclerotic cardiovascular disease (ASCVD). However, the performance of the Pooled Cohort Equations (PCE) remains uncertain in SAs living in the US. We aimed to study the interplay between predicted 10-year ASCVD risk and coronary artery calcium (CAC) in SAs compared to other racial/ethnic groups.
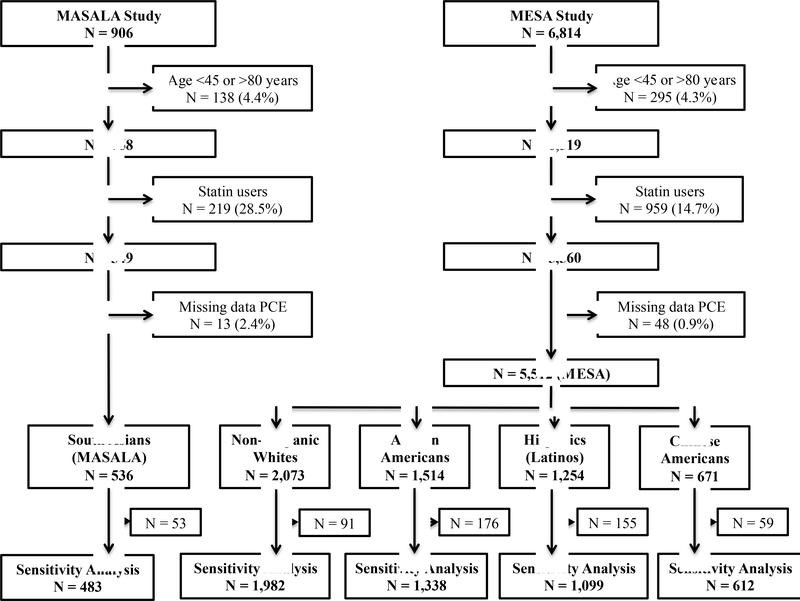
Methods: We studied 536 SAs from the Mediators of Atherosclerosis in South Asians Living in America (MASALA) study, and 2073 Non-Hispanic Whites (NHWs), 1514 African Americans (AAs), 1254 Hispanics, and 671 Chinese Americans (CAs) from the Multi-Ethnic Study of Atherosclerosis (MESA) who were not currently on statins. We used logistic regression models to assess the association between race/ethnicity and CAC within each ASCVD risk stratum.
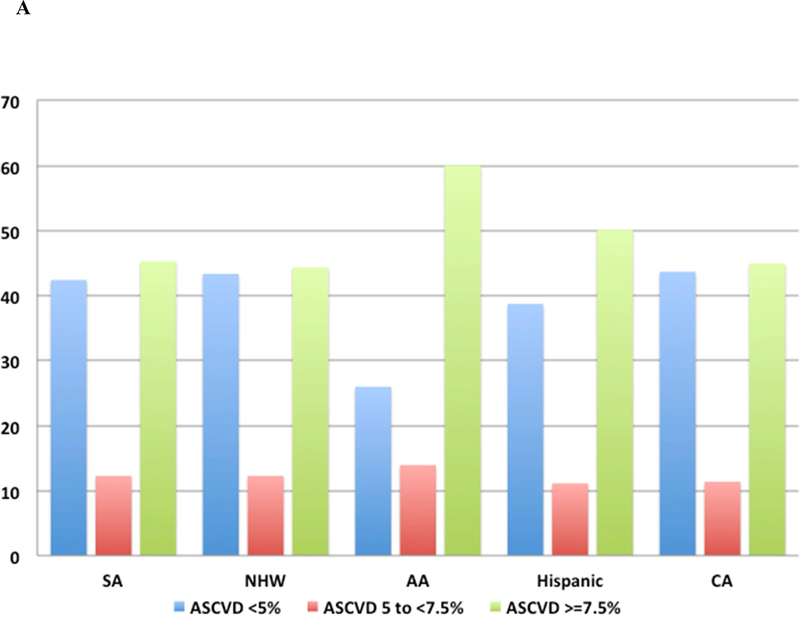
Results: SAs at low and at intermediate estimated ASCVD risk were more likely to have CAC = 0 compared to NHWs, while SAs at high risk had a similar CAC burden to NHWs. For example, intermediate-risk SAs had a 73% higher odds of CAC = 0 compared to NHWs (95% 1.00-2.99), while high-risk SAs were equally likely to have CAC = 0 (OR 0.95, 95% CI 0.65-1.38) and CAC >100 (OR 0.86, 95% CI 0.61-1.22).
Conclusions: Our results suggest that the extent of ASCVD risk overestimation using the PCEs may be even greater among SAs considered at low and intermediate risk than among NHWs. Studies with incident ASCVD events are required to validate and/or recalibrate current ASCVD risk prediction tools in this group.
Keywords: Atherosclerosis; Cardiovascular disease; Coronary artery calcium; Race/ethnicity; Risk; South Asian.
Copyright © 2018 Elsevier B.V. All rights reserved.
Conflict of interest statement
CONFLICT OF INTEREST
The authors declared they do not have anything to disclose regarding conflict of interest with respect to this manuscript.
Figures
Comment in
-
Time for risk assessment without borders.Atherosclerosis. 2018 Dec;279:93-94. doi: 10.1016/j.atherosclerosis.2018.10.019. Epub 2018 Oct 21. Atherosclerosis. 2018. PMID: 30401495 No abstract available.
Similar articles
-
Association of cardiovascular health with subclinical coronary atherosclerosis progression among five racial and ethnic groups: The MASALA and MESA studies.Atherosclerosis. 2024 May;392:117522. doi: 10.1016/j.atherosclerosis.2024.117522. Epub 2024 Mar 17. Atherosclerosis. 2024. PMID: 38583288 Free PMC article.
-
Implications of the 2019 American College of Cardiology/American Heart Association Primary Prevention Guidelines and potential value of the coronary artery calcium score among South Asians in the US: The Mediators of Atherosclerosis in South Asians Living in America (MASALA) study.Atherosclerosis. 2021 Oct;334:48-56. doi: 10.1016/j.atherosclerosis.2021.08.030. Epub 2021 Aug 23. Atherosclerosis. 2021. PMID: 34481175 Free PMC article.
-
Ectopic Fat Depots and Coronary Artery Calcium in South Asians Compared With Other Racial/Ethnic Groups.J Am Heart Assoc. 2016 Nov 17;5(11):e004257. doi: 10.1161/JAHA.116.004257. J Am Heart Assoc. 2016. PMID: 27856485 Free PMC article.
-
Coronary artery calcification and ethnicity.J Cardiovasc Comput Tomogr. 2019 Nov-Dec;13(6):353-359. doi: 10.1016/j.jcct.2018.10.002. Epub 2018 Oct 2. J Cardiovasc Comput Tomogr. 2019. PMID: 30322775 Review.
-
Association of Coronary Artery Calcium Density and Volume With Predicted Atherosclerotic Cardiovascular Disease Risk and Cardiometabolic Risk Factors in South Asians: The Mediators of Atherosclerosis in South Asians Living in America (MASALA) Study.Curr Probl Cardiol. 2023 Apr;48(4):101105. doi: 10.1016/j.cpcardiol.2022.101105. Epub 2022 Jan 7. Curr Probl Cardiol. 2023. PMID: 34999157 Free PMC article. Review.
Cited by
-
Identification and Management of Atherosclerotic Cardiovascular Disease Risk in South Asian Populations in the U.S.JACC Adv. 2023 Mar;2(2):100258. doi: 10.1016/j.jacadv.2023.100258. Epub 2023 Mar 31. JACC Adv. 2023. PMID: 38089916 Free PMC article.
-
Metabolite Profiles of Plant-Based Diets and Cardiometabolic Risk in the Mediators of Atherosclerosis in South Asians Living in America Study.J Nutr. 2024 Aug;154(8):2501-2513. doi: 10.1016/j.tjnut.2024.06.007. Epub 2024 Jun 19. J Nutr. 2024. PMID: 38901635 Free PMC article.
-
Atherosclerostic cardiovascular disease risk score: Are Indians underestimating the risk of cardiovascular disease?Indian Heart J. 2019 Jul-Aug;71(4):364-365. doi: 10.1016/j.ihj.2019.08.002. Epub 2019 Aug 30. Indian Heart J. 2019. PMID: 31779868 Free PMC article. No abstract available.
-
Coronary Artery Calcium for Risk Stratification of Sudden Cardiac Death: The Coronary Artery Calcium Consortium.JACC Cardiovasc Imaging. 2022 Jul;15(7):1259-1270. doi: 10.1016/j.jcmg.2022.02.011. Epub 2022 Mar 21. JACC Cardiovasc Imaging. 2022. PMID: 35370113 Free PMC article.
-
Primary and Secondary Prevention of CAD: A Review.Int J Angiol. 2021 Dec 24;31(1):16-26. doi: 10.1055/s-0041-1729925. eCollection 2022 Mar. Int J Angiol. 2021. PMID: 35221848 Free PMC article.
References
-
- Hoeffel Elizabeth M.; Rastogi Sonya ; Kim Myoung Ouk; Shahid H The Asian Population: 2010. 2012.
-
- Anand SS, Yusuf S, Vuksan V, et al. Differences in risk factors, atherosclerosis, and cardiovascular disease between ethnic groups in Canada: the Study of Health Assessment and Risk in Ethnic groups (SHARE). Lancet (London, England) 2000; 356: 279–84. - PubMed
-
- Chambers JC, Eda S, Bassett P, et al. C-reactive protein, insulin resistance, central obesity, and coronary heart disease risk in Indian Asians from the United Kingdom compared with European whites. Circulation 2001; 104: 145–50. - PubMed
-
- Palaniappan L, Wang Y, Fortmann SP. Coronary heart disease mortality for six ethnic groups in California, 1990–2000. Ann Epidemiol 2004; 14: 499–506. - PubMed
-
- Khan NA, Grubisic M, Hemmelgarn B, Humphries K, King KM, Quan H. Outcomes After Acute Myocardial Infarction in South Asian, Chinese, and White Patients. Circulation 2010; 122: 1570–7. - PubMed
Publication types
MeSH terms
Grants and funding
- N01 HC095161/HL/NHLBI NIH HHS/United States
- K23 HL080026/HL/NHLBI NIH HHS/United States
- N01 HC095167/HL/NHLBI NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- K24 HL112827/HL/NHLBI NIH HHS/United States
- P30 DK098722/DK/NIDDK NIH HHS/United States
- UL1 TR001420/TR/NCATS NIH HHS/United States
- N01 HC095163/HL/NHLBI NIH HHS/United States
- P30 DK092924/DK/NIDDK NIH HHS/United States
- N01 HC095166/HL/NHLBI NIH HHS/United States
- N01 HC095160/HL/NHLBI NIH HHS/United States
- N01 HC095168/HL/NHLBI NIH HHS/United States
- R01 HL093009/HL/NHLBI NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- N01 HC095162/HL/NHLBI NIH HHS/United States
- P30 DK092949/DK/NIDDK NIH HHS/United States
- N01 HC095165/HL/NHLBI NIH HHS/United States
- N01 HC095164/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
