

Tailored approaches grounded on immunogenetic features for refined prognostication in chronic lymphocytic leukemia
- PMID: 30262567
- PMCID: PMC6355487
- DOI: 10.3324/haematol.2018.195032
Tailored approaches grounded on immunogenetic features for refined prognostication in chronic lymphocytic leukemia
Abstract
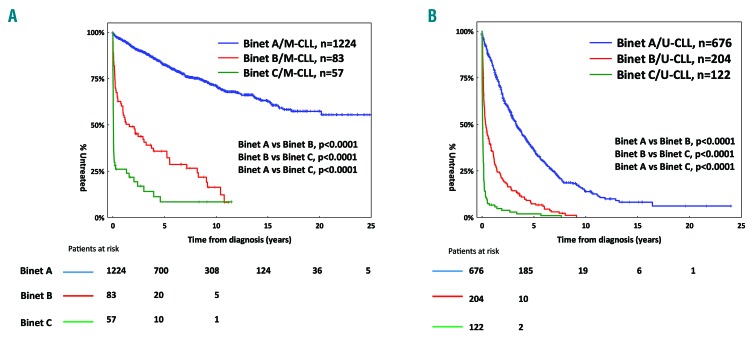
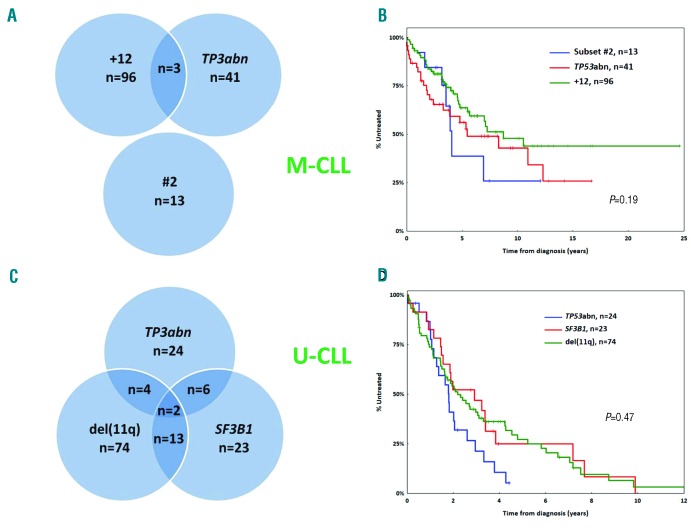
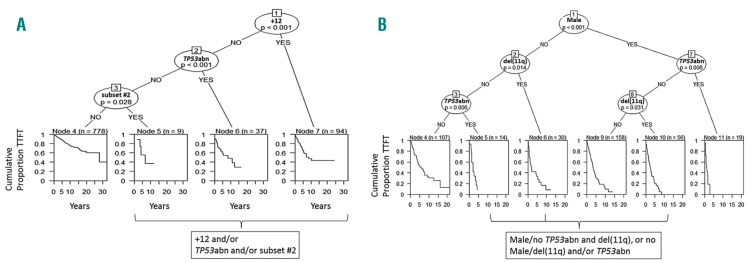
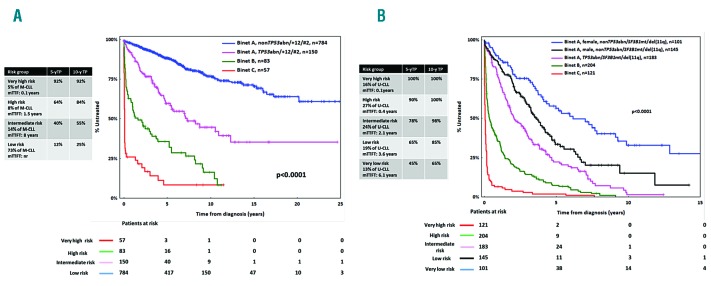
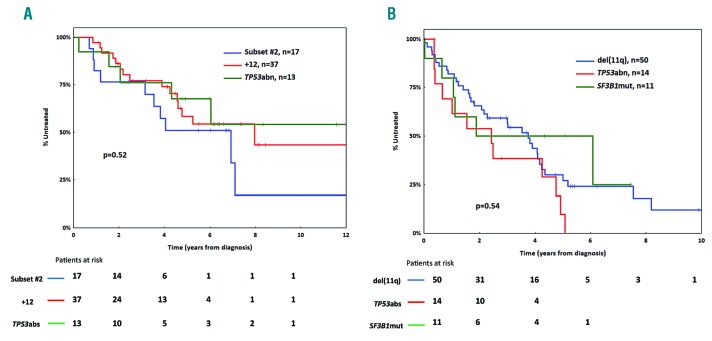
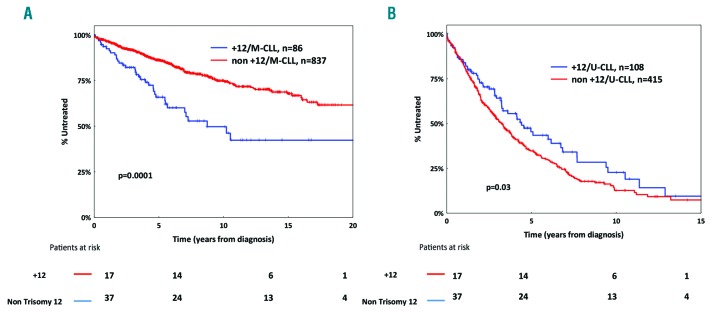
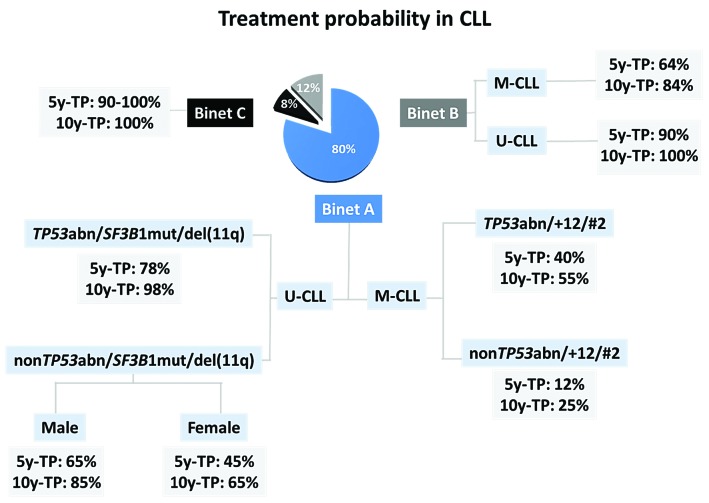
Chronic lymphocytic leukemia (CLL) patients with differential somatic hypermutation status of the immunoglobulin heavy variable genes, namely mutated or unmutated, display fundamental clinico-biological differences. Considering this, we assessed prognosis separately within mutated (M-CLL) and unmutated (U-CLL) CLL in 3015 patients, hypothesizing that the relative significance of relevant indicators may differ between these two categories. Within Binet A M-CLL patients, besides TP53 abnormalities, trisomy 12 and stereotyped subset #2 membership were equivalently associated with the shortest time-to-first-treatment and a treatment probability at five and ten years after diagnosis of 40% and 55%, respectively; the remaining cases exhibited 5-year and 10-year treatment probability of 12% and 25%, respectively. Within Binet A U-CLL patients, besides TP53 abnormalities, del(11q) and/or SF3B1 mutations were associated with the shortest time-to-first-treatment (5- and 10-year treatment probability: 78% and 98%, respectively); in the remaining cases, males had a significantly worse prognosis than females. In conclusion, the relative weight of indicators that can accurately risk stratify early-stage CLL patients differs depending on the somatic hypermutation status of the immunoglobulin heavy variable genes of each patient. This finding highlights the fact that compartmentalized approaches based on immunogenetic features are necessary to refine and tailor prognostication in CLL.
Copyright © 2019 Ferrata Storti Foundation.
Figures
References
-
- Binet JL, Auquier A, Dighiero G, et al. A new prognostic classification of chronic lymphocytic leukemia derived from a multivariate survival analysis. Cancer. 1981;48(1):198–206. - PubMed
-
- Rai KR, Sawitsky A, Cronkite EP, Chanana AD, Levy RN, Pasternack BS. Clinical staging of chronic lymphocytic leukemia. Blood. 1975;46(2):219–234. - PubMed
-
- Cramer P, Hallek M. Prognostic factors in chronic lymphocytic leukemia-what do we need to know¿ Nat Rev Clin Oncol. 2011;8(1):38–47. - PubMed
-
- Gentile M, Mauro FR, Rossi D, et al. Italian external and multicentric validation of the MD Anderson Cancer Center nomogram and prognostic index for chronic lymphocytic leukaemia patients: analysis of 1502 cases. Br J Haematol. 2014;167(2):224–232. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
