

Chromosome Y-encoded antigens associate with acute graft-versus-host disease in sex-mismatched stem cell transplant
- PMID: 30262602
- PMCID: PMC6177651
- DOI: 10.1182/bloodadvances.2018019513
Chromosome Y-encoded antigens associate with acute graft-versus-host disease in sex-mismatched stem cell transplant
Abstract
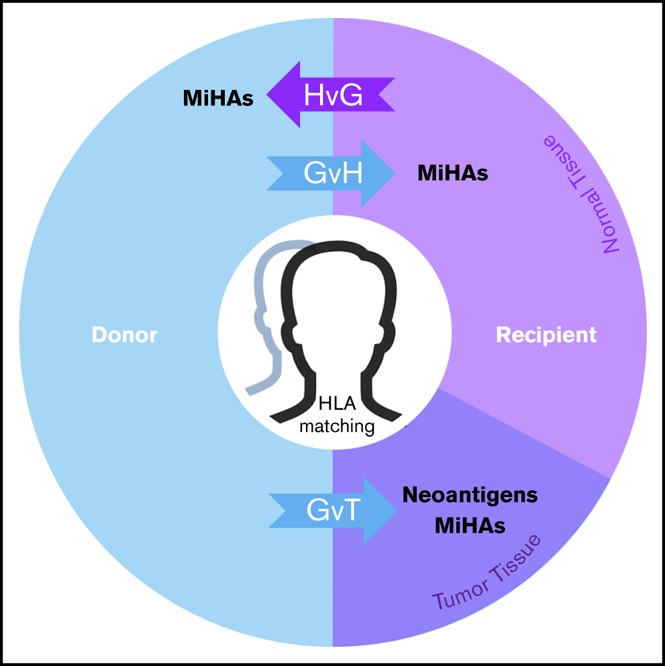
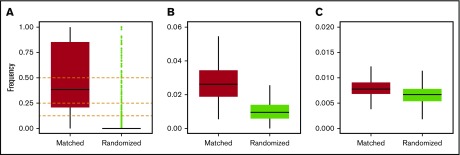
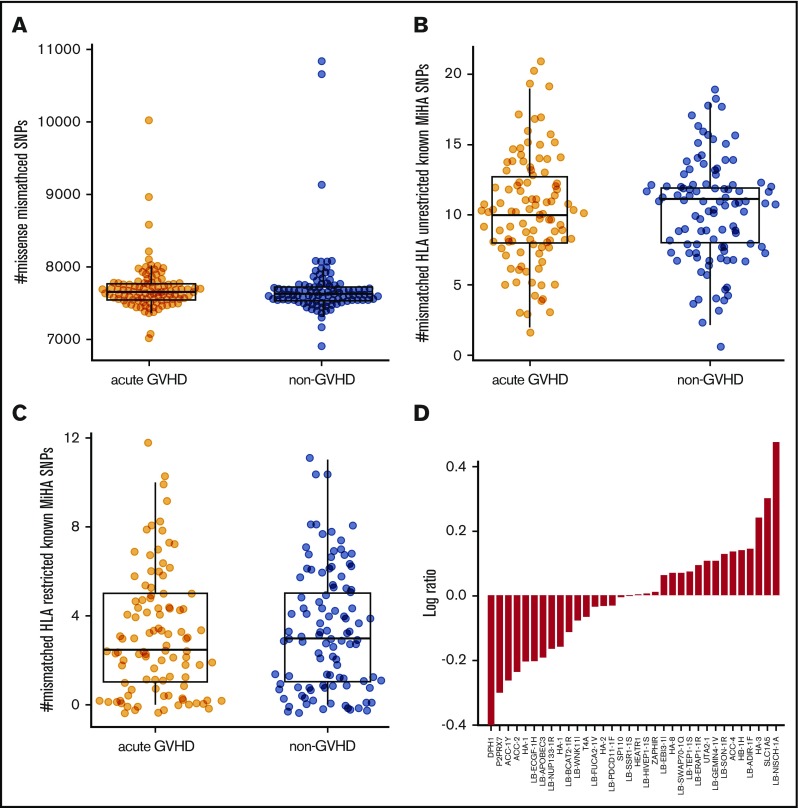
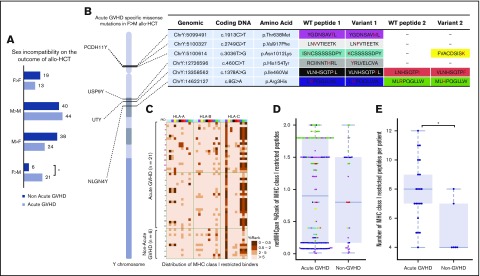
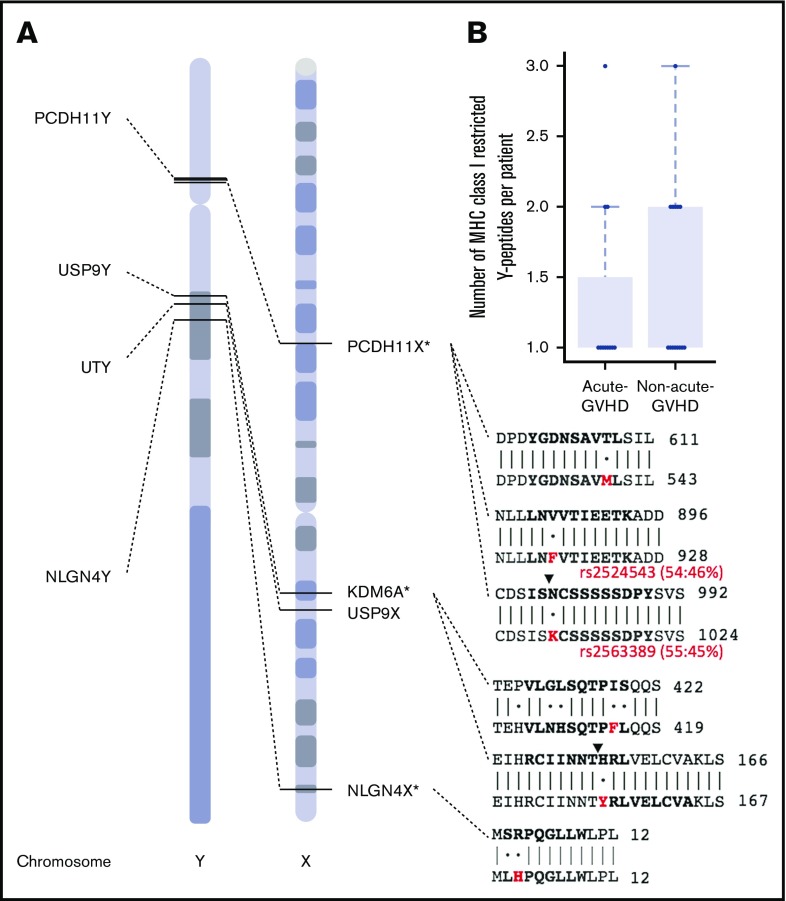
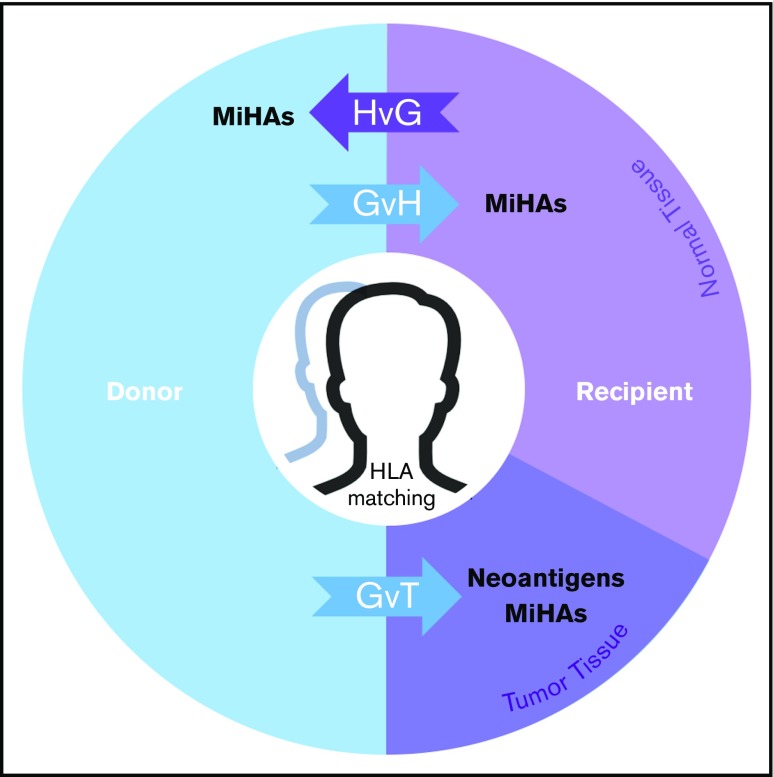
Allogeneic hematopoietic stem cell transplantation (allo-HCT) is a curative option for blood cancers, but the coupled effects of graft-versus-tumor and graft-versus-host disease (GVHD) limit its broader application. Outcomes improve with matching at HLAs, but other factors are required to explain residual risk of GVHD. In an effort to identify genetic associations outside the major histocompatibility complex, we conducted a genome-wide clinical outcomes study on 205 acute myeloid leukemia patients and their fully HLA-A-, HLA-B-, HLA-C-, HLA-DRB1-, and HLA-DQB1-matched (10/10) unrelated donors. HLA-DPB1 T-cell epitope permissibility mismatches were observed in less than half (45%) of acute GVHD cases, motivating a broader search for genetic factors affecting clinical outcomes. A novel bioinformatics workflow adapted from neoantigen discovery found no associations between acute GVHD and known, HLA-restricted minor histocompatibility antigens (MiHAs). These results were confirmed with microarray data from an additional 988 samples. On the other hand, Y-chromosome-encoded single-nucleotide polymorphisms in 4 genes (PCDH11Y, USP9Y, UTY, and NLGN4Y) did associate with acute GVHD in male patients with female donors. Males in this category with acute GVHD had more Y-encoded variant peptides per patient with higher predicted HLA-binding affinity than males without GVHD who matched X-paralogous alleles in their female donors. Methods and results described here have an immediate impact for allo-HCT, warranting further development and larger genomic studies where MiHAs are clinically relevant, including cancer immunotherapy, solid organ transplant, and pregnancy.
© 2018 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: W.B. is an employee of Human Longevity, Inc. N.M.P. is founder of Root Deep Insight, Inc., a personal immunogenomics company. The remaining authors declare no competing financial interests.
Figures
Similar articles
-
Genome-wide minor histocompatibility matching as related to the risk of graft-versus-host disease.Blood. 2017 Feb 9;129(6):791-798. doi: 10.1182/blood-2016-09-737700. Epub 2016 Nov 21. Blood. 2017. PMID: 27872059 Free PMC article.
-
Degree of predicted minor histocompatibility antigen mismatch correlates with poorer clinical outcomes in nonmyeloablative allogeneic hematopoietic cell transplantation.Biol Blood Marrow Transplant. 2010 Oct;16(10):1370-81. doi: 10.1016/j.bbmt.2010.03.022. Epub 2010 Mar 28. Biol Blood Marrow Transplant. 2010. PMID: 20353833
-
Multicenter analyses demonstrate significant clinical effects of minor histocompatibility antigens on GvHD and GvL after HLA-matched related and unrelated hematopoietic stem cell transplantation.Biol Blood Marrow Transplant. 2013 Aug;19(8):1244-53. doi: 10.1016/j.bbmt.2013.06.001. Epub 2013 Jun 10. Biol Blood Marrow Transplant. 2013. PMID: 23756210
-
Minor histocompatibility antigens to predict, monitor or manipulate GvL and GvHD after allogeneic hematopoietic cell transplantation.Best Pract Res Clin Haematol. 2024 Jun;37(2):101555. doi: 10.1016/j.beha.2024.101555. Epub 2024 May 15. Best Pract Res Clin Haematol. 2024. PMID: 39098803 Review.
-
Alloreactivity as therapeutic principle in the treatment of hematologic malignancies. Studies of clinical and immunologic aspects of allogeneic hematopoietic cell transplantation with nonmyeloablative conditioning.Dan Med Bull. 2007 May;54(2):112-39. Dan Med Bull. 2007. PMID: 17521527 Review.
Cited by
-
Computational Analysis of HLA-presentation of Non-synonymous Recipient Mismatches Indicates Effect on the Risk of Chronic Graft-vs.-Host Disease After Allogeneic HSCT.Front Immunol. 2019 Jul 16;10:1625. doi: 10.3389/fimmu.2019.01625. eCollection 2019. Front Immunol. 2019. PMID: 31379830 Free PMC article.
-
Genetics of HLA Peptide Presentation and Impact on Outcomes in HLA-Matched Allogeneic Hematopoietic Cell Transplantation.Transplant Cell Ther. 2021 Jul;27(7):591-599. doi: 10.1016/j.jtct.2021.04.003. Epub 2021 Apr 18. Transplant Cell Ther. 2021. PMID: 33882342 Free PMC article.
-
Secondary bone marrow graft loss after third-party virus-specific T cell infusion: Case report of a rare complication.Nat Commun. 2024 Mar 29;15(1):2749. doi: 10.1038/s41467-024-47056-3. Nat Commun. 2024. PMID: 38553461 Free PMC article.
-
Sexual dimorphism in neurological function after SCI is associated with disrupted neuroinflammation in both injured spinal cord and brain.Brain Behav Immun. 2022 Mar;101:1-22. doi: 10.1016/j.bbi.2021.12.017. Epub 2021 Dec 23. Brain Behav Immun. 2022. PMID: 34954073 Free PMC article.
-
HTLV-1 infection of donor-derived T cells might promote acute graft-versus-host disease following liver transplantation.Nat Commun. 2022 Nov 30;13(1):7368. doi: 10.1038/s41467-022-35111-w. Nat Commun. 2022. PMID: 36450748 Free PMC article.
References
-
- Copelan EA. Hematopoietic stem-cell transplantation. N Engl J Med. 2006;354(17):1813-1826. - PubMed
-
- Horowitz MM, Gale RP, Sondel PM, et al. . Graft-versus-leukemia reactions after bone marrow transplantation. Blood. 1990;75(3):555-562. - PubMed
-
- Miller JS, Warren EH, van den Brink MR, et al. . NCI First International Workshop on The Biology, Prevention, and Treatment of Relapse After Allogeneic Hematopoietic Stem Cell Transplantation: report from the Committee on the Biology Underlying Recurrence of Malignant Disease following Allogeneic HSCT: graft-versus-tumor/leukemia reaction. Biol Blood Marrow Transplant. 2010;16(5):565-586. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
