

Effect of Algorithm-Based Therapy vs Usual Care on Clinical Success and Serious Adverse Events in Patients with Staphylococcal Bacteremia: A Randomized Clinical Trial
- PMID: 30264119
- PMCID: PMC6233609
- DOI: 10.1001/jama.2018.13155
Effect of Algorithm-Based Therapy vs Usual Care on Clinical Success and Serious Adverse Events in Patients with Staphylococcal Bacteremia: A Randomized Clinical Trial
Abstract
Importance: The appropriate duration of antibiotics for staphylococcal bacteremia is unknown.
Objective: To test whether an algorithm that defines treatment duration for staphylococcal bacteremia vs standard of care provides noninferior efficacy without increasing severe adverse events.
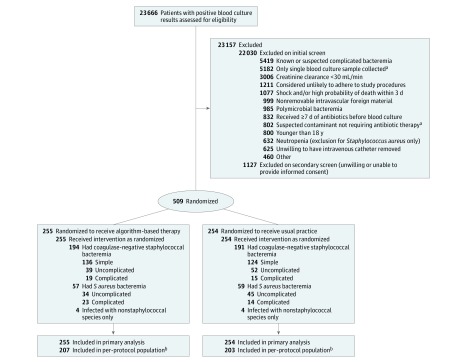
Design, setting, and participants: A randomized trial involving adults with staphylococcal bacteremia was conducted at 16 academic medical centers in the United States (n = 15) and Spain (n = 1) from April 2011 to March 2017. Patients were followed up for 42 days beyond end of therapy for those with Staphylococcus aureus and 28 days for those with coagulase-negative staphylococcal bacteremia. Eligible patients were 18 years or older and had 1 or more blood cultures positive for S aureus or coagulase-negative staphylococci. Patients were excluded if they had known or suspected complicated infection at the time of randomization.
Interventions: Patients were randomized to algorithm-based therapy (n = 255) or usual practice (n = 254). Diagnostic evaluation, antibiotic selection, and duration of therapy were predefined for the algorithm group, whereas clinicians caring for patients in the usual practice group had unrestricted choice of antibiotics, duration, and other aspects of clinical care.
Main outcomes and measures: Coprimary outcomes were (1) clinical success, as determined by a blinded adjudication committee and tested for noninferiority within a 15% margin; and (2) serious adverse event rates in the intention-to-treat population, tested for superiority. The prespecified secondary outcome measure, tested for superiority, was antibiotic days among per-protocol patients with simple or uncomplicated bacteremia.
Results: Among the 509 patients randomized (mean age, 56.6 [SD, 16.8] years; 226 [44.4%] women), 480 (94.3%) completed the trial. Clinical success was documented in 209 of 255 patients assigned to algorithm-based therapy and 207 of 254 randomized to usual practice (82.0% vs 81.5%; difference, 0.5% [1-sided 97.5% CI, -6.2% to ∞]). Serious adverse events were reported in 32.5% of algorithm-based therapy patients and 28.3% of usual practice patients (difference, 4.2% [95% CI, -3.8% to 12.2%]). Among per-protocol patients with simple or uncomplicated bacteremia, mean duration of therapy was 4.4 days for algorithm-based therapy vs 6.2 days for usual practice (difference, -1.8 days [95% CI, -3.1 to -0.6]).
Conclusions and relevance: Among patients with staphylococcal bacteremia, the use of an algorithm to guide testing and treatment compared with usual care resulted in a noninferior rate of clinical success. Rates of serious adverse events were not significantly different, but interpretation is limited by wide confidence intervals. Further research is needed to assess the utility of the algorithm.
Trial registration: ClinicalTrials.gov Identifier: NCT01191840.
Conflict of interest statement
Figures
Comment in
-
Treatment Algorithms for Staphylococcal Bacteremia: Improving Clinical Care and Enhancing Antimicrobial Stewardship.JAMA. 2018 Sep 25;320(12):1243-1244. doi: 10.1001/jama.2018.13315. JAMA. 2018. PMID: 30264099 No abstract available.
References
-
- Diekema DJ, Pfaller MA, Schmitz FJ, et al. ; SENTRY Participants Group . Survey of infections due to Staphylococcus species: frequency of occurrence and antimicrobial susceptibility of isolates collected in the United States, Canada, Latin America, Europe, and the Western Pacific region for the SENTRY Antimicrobial Surveillance Program, 1997-1999. Clin Infect Dis. 2001;32(suppl 2):S114-S132. doi: 10.1086/320184 - DOI - PubMed
-
- Liu C, Bayer A, Cosgrove SE, et al. ; Infectious Diseases Society of America . Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clin Infect Dis. 2011;52(3):e18-e55. doi: 10.1093/cid/ciq146 - DOI - PubMed
-
- Mermel LA, Allon M, Bouza E, et al. Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 update by the Infectious Diseases Society of America [published correction appears in Clin Infect Dis. 2010;50(7):1079]. Clin Infect Dis. 2009;49(1):1-45. doi: 10.1086/599376 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
