

Prevalence of Parent-Reported Traumatic Brain Injury in Children and Associated Health Conditions
- PMID: 30264150
- PMCID: PMC6248161
- DOI: 10.1001/jamapediatrics.2018.2740
Prevalence of Parent-Reported Traumatic Brain Injury in Children and Associated Health Conditions
Abstract
Importance: Traumatic brain injury (TBI) in children results in a high number of emergency department visits and risk for long-term adverse effects.
Objectives: To estimate lifetime prevalence of TBI in a nationally representative sample of US children and describe the association between TBI and other childhood health conditions.
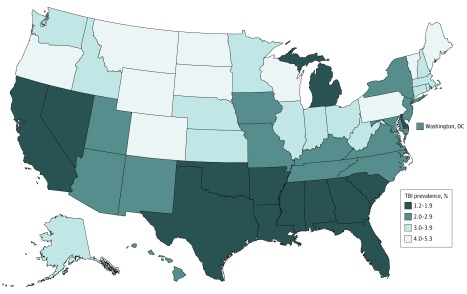
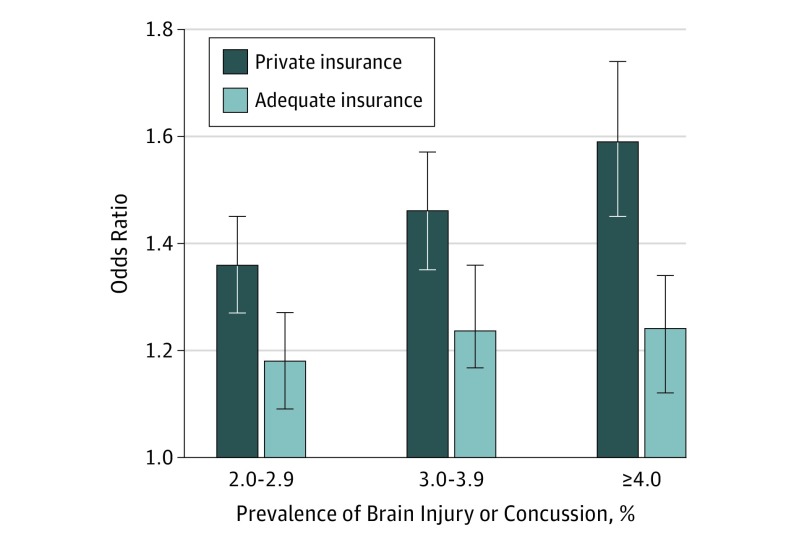
Design, setting, and participants: Data were analyzed from the 2011-2012 National Survey of Children's Health, a cross-sectional telephone survey of US households with a response rate of 23%. Traumatic brain injury prevalence estimates were stratified by sociodemographic characteristics. The likelihood of reporting specific health conditions was compared between children with and without TBI. Age-adjusted prevalence estimates were computed for each state. Associations between TBI prevalence, insurance type, and parent rating of insurance adequacy were examined. Data analysis was conducted from February 1, 2016, through November 1, 2017.
Main outcomes and measures: Lifetime estimate of TBI in children, associated childhood health conditions, and parent report of health insurance type and adequacy.
Results: The lifetime estimate of parent-reported TBI among children was 2.5% (95% CI, 2.3%-2.7%), representing over 1.8 million children nationally. Children with a lifetime history of TBI were more likely to have a variety of health conditions compared with those without a TBI history. Those with the highest prevalence included learning disorders (21.4%; 95% CI, 18.1%-25.2%); attention-deficit/hyperactivity disorder (20.5%; 95% CI, 17.4%-24.0%); speech/language problems (18.6%; 95% CI, 15.8%-21.7%); developmental delay (15.3%; 95% CI, 12.9%-18.1%); bone, joint, or muscle problems (14.2%; 95% CI, 11.6%-17.2%); and anxiety problems (13.2%; 95% CI, 11.0%-16.0%). States with a higher prevalence of childhood TBI were more likely to have a higher proportion of children with private health insurance and higher parent report of adequate insurance. Examples of states with higher prevalence of TBI and higher proportion of private insurance included Maine, Vermont, Pennsylvania, Washington, Montana, Wyoming North Dakota, South Dakota, and Colorado.
Conclusions and relevance: A large number of US children have experienced a TBI during childhood. Higher TBI prevalence in states with greater levels of private insurance and insurance adequacy may suggest an underrecognition of TBI among children with less access to care. For more comprehensive monitoring, health care professionals should be aware of the increased risk of associated health conditions among children with TBI.
Conflict of interest statement
Figures
Comment in
-
Variation in National Survey Estimates and Youth Traumatic Brain Injury-Where Does the Truth Lie?JAMA Pediatr. 2019 Apr 1;173(4):399. doi: 10.1001/jamapediatrics.2019.0001. JAMA Pediatr. 2019. PMID: 30801620 No abstract available.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
