

The Impact of Population-Based Disease Management Services on Health Care Utilisation and Costs: Results of the CAPICHe Trial
- PMID: 30264259
- PMCID: PMC6318195
- DOI: 10.1007/s11606-018-4682-5
The Impact of Population-Based Disease Management Services on Health Care Utilisation and Costs: Results of the CAPICHe Trial
Abstract
Background: Disease management programmes may improve quality of care, improve health outcomes and potentially reduce total healthcare costs. To date, only one very large population-based study has been undertaken and indicated reductions in hospital admissions > 10%.
Objective: We sought to confirm the effectiveness of population-based disease management programmes. The objective of this study was to evaluate the relative impact on healthcare utilisation and cost of participants the Costs to Australian Private Insurance - Coaching Health (CAPICHe) trial.
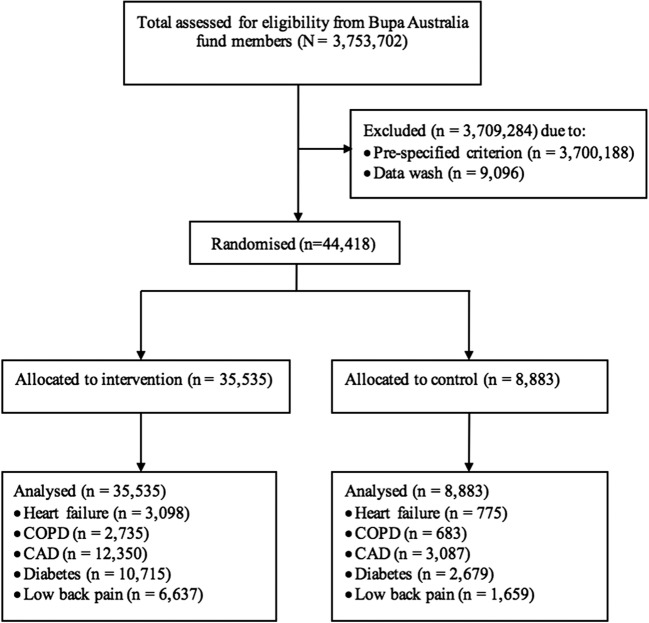
Design: Parallel-group randomised controlled trial, intention-to-treat analysis SETTING: Australian population PARTICIPANTS: Forty-four thousand four hundred eighteen individuals (18-90 years of age) with private health insurance and diagnosis of heart failure, chronic obstructive pulmonary disease (COPD), coronary artery disease (CAD), diabetes, or low back pain, with predicted high cost claims for the following 12 months.
Intervention: Health coaching for disease management from Bupa Health Dialog, vs Usual Care.
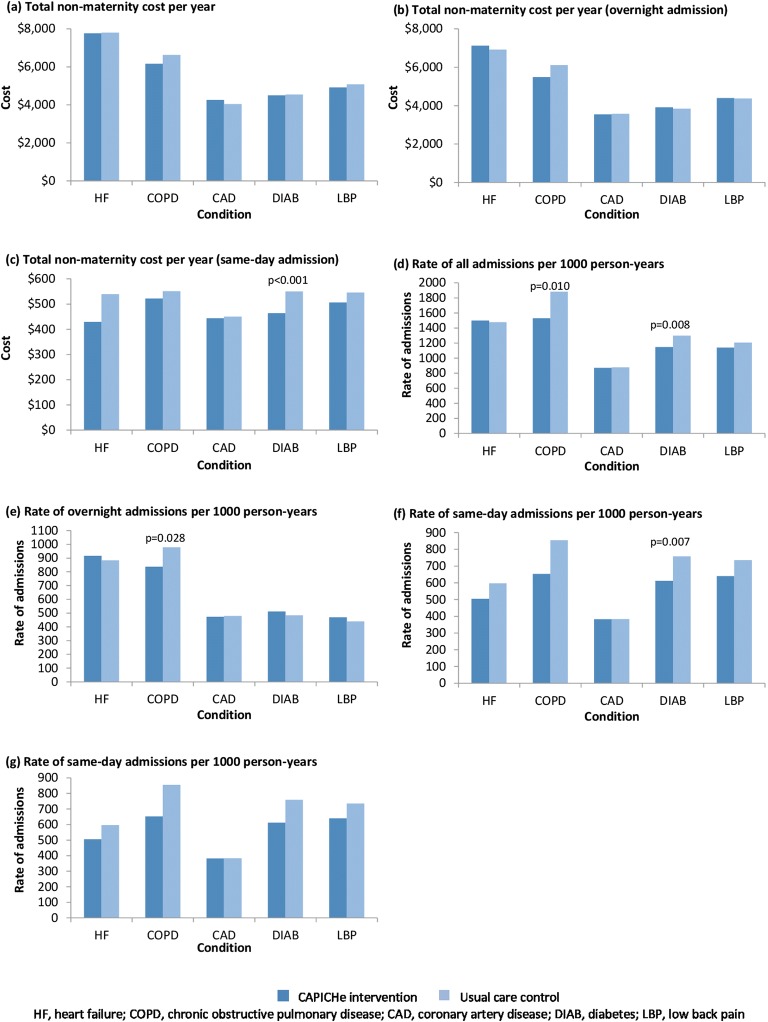
Main outcome measures: Total cost of claims per member to the private health insurer 1 year post-randomisation for hospital admissions, including same-day, medical and prostheses hospital claims, excluding any maternity costs. Analysis was based on the intent-to-treat population.
Results: Estimated total cost 1 year post-randomisation was not significantly different (means: intervention group A$4934; 95% CI A$4823-A$5045 vs control group A$4868; 95% CI A$4680-A$5058; p = 0.524). However, the intervention group had significantly lower same-day admission costs (A$468; 95% CI A$454-A$482 vs A$508; 95% CI A$484-A$533; p = 0.002) and fewer same-day admissions per 1000 person-years (intervention group, 530; 95% CI 508-552 vs control group, 614; 95% CI 571-657; p = 0.002). Subgroup analyses indicated that the intervention group had significantly fewer admissions for patients with COPD and fewer same-day admissions for patients with diabetes.
Conclusions: Chronic disease health coaching was not effective to reduce the total cost after 12 months of follow-up for higher risk individuals with a chronic condition. Statistically significant changes were found with fewer same-day admissions; however, these did not translate into cost savings from a private health insurance perspective.
Keywords: costs; disease management; insurance; private healthcare.
Conflict of interest statement
PS, JB and SN were independent consultants and have no conflicts of interest. CP and SG are employees of Bupa Australia. DC is an employee of Bupa Health Dialog, part of Bupa Australia. Coaching was provided by Bupa Health Dialog. Health Dialog in the USA provided the risk scoring algorithm which was adapted for Australia.
Figures
Comment in
-
Keeping Pace with the Expanding Role of Health Coaching.J Gen Intern Med. 2019 Jan;34(1):5-6. doi: 10.1007/s11606-018-4730-1. J Gen Intern Med. 2019. PMID: 30406571 Free PMC article. No abstract available.
References
-
- Todd W, Nash D, editors. Disease Management: A Systems Approach to Improving Patient Outcomes. San Francisco: Jossey Bass; 2001.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
