

Repetitive transcranial magnetic stimulation therapy for motor recovery in Parkinson's disease: A Meta-analysis
- PMID: 30264518
- PMCID: PMC6236247
- DOI: 10.1002/brb3.1132
Repetitive transcranial magnetic stimulation therapy for motor recovery in Parkinson's disease: A Meta-analysis
Abstract
Introduction: Therapeutic effects of repetitive transcranial magnetic stimulation (rTMS) on motor recovery of Parkinson's disease (PD) have been reported; however, the protocols of these studies varied greatly. The aim of this meta-analysis was to evaluate the optimal rTMS parameters for motor recovery of PD.
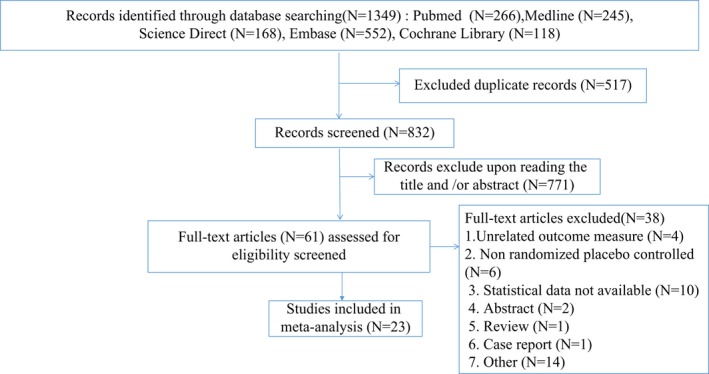
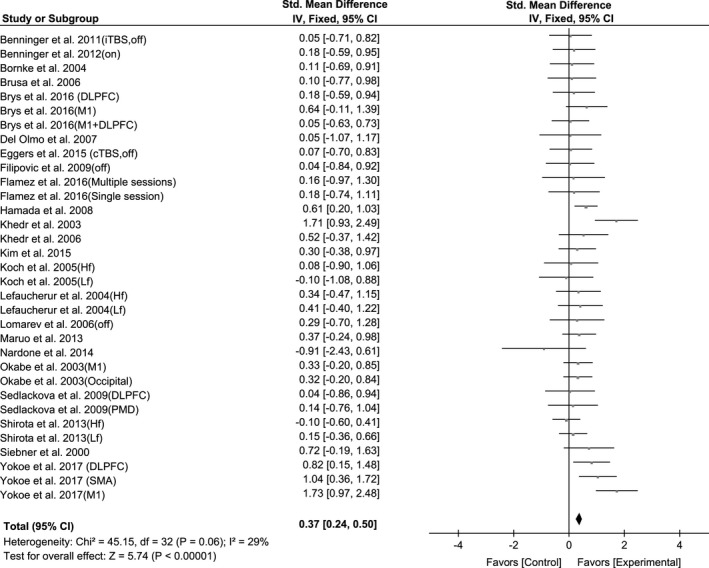
Methods: Electronic databases were searched for studies investigating the therapeutic effects of rTMS on motor function in patients with PD. The section III of the Unified Parkinson's Disease Rating Scale (UPDRS) was extracted as the primary outcome, and the standardized mean difference (SMD) with 95% confidence interval (CI) was calculated.
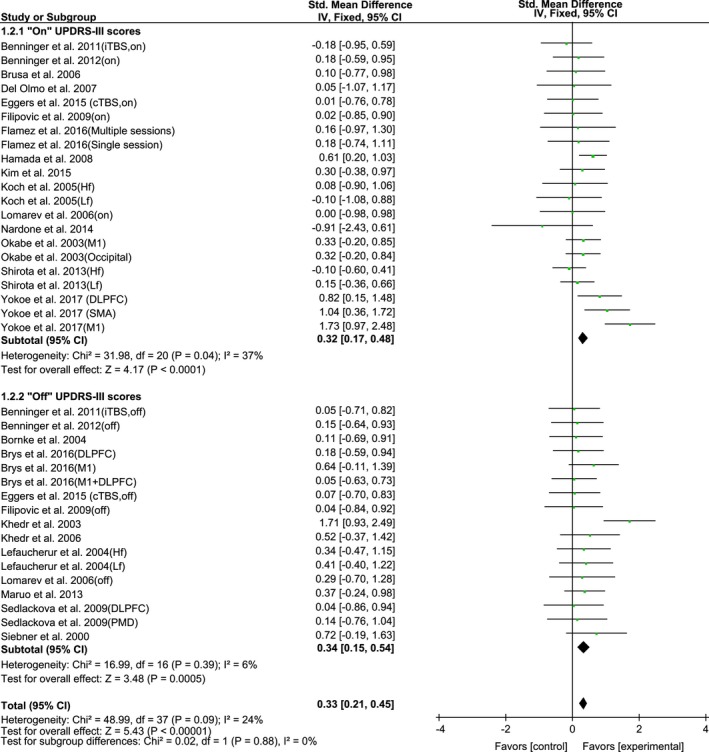
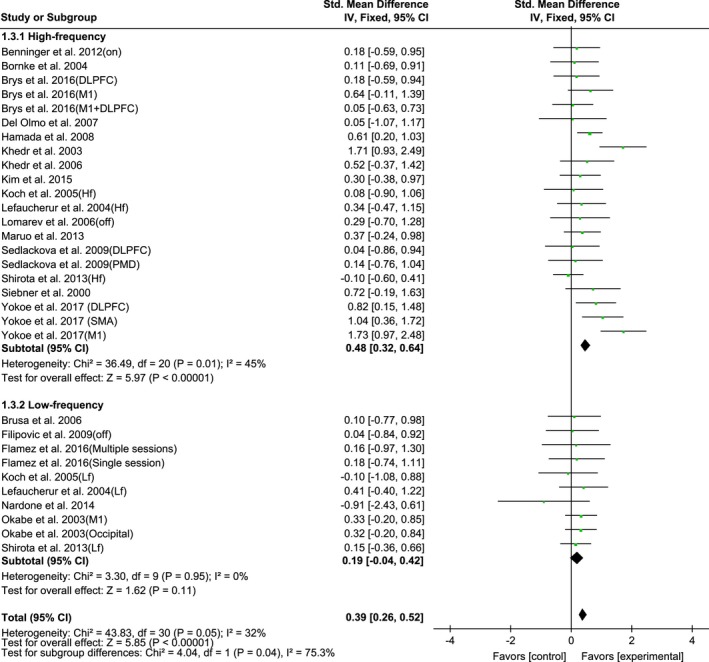
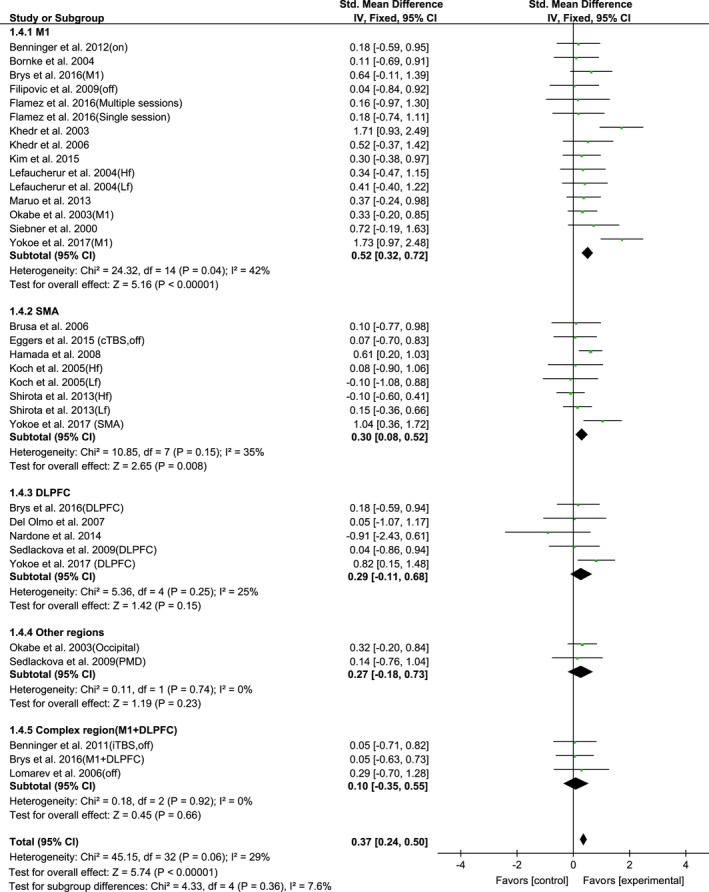
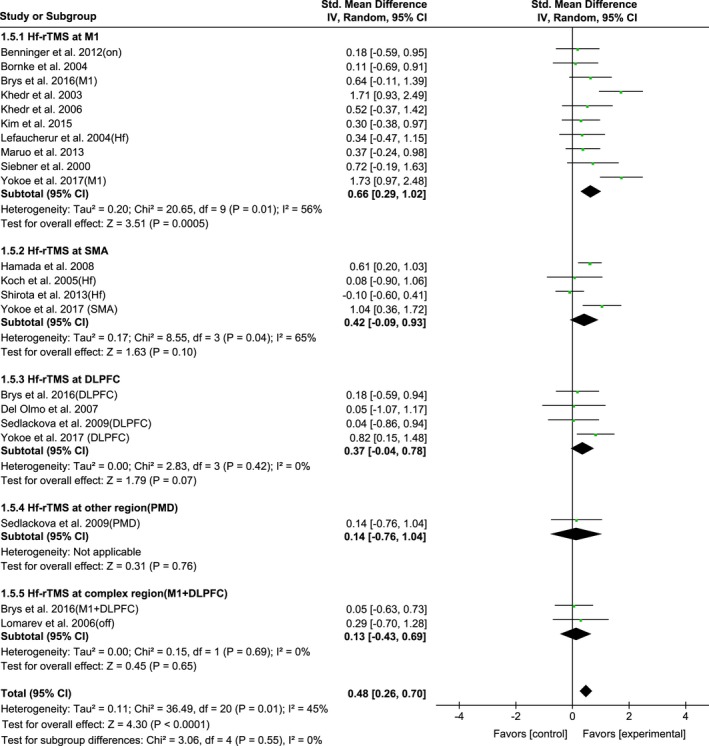
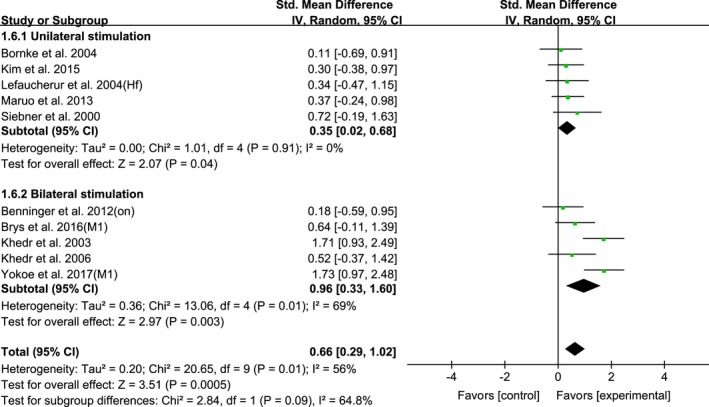
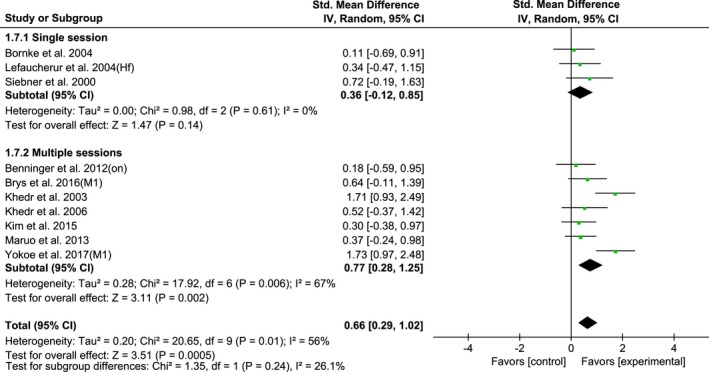
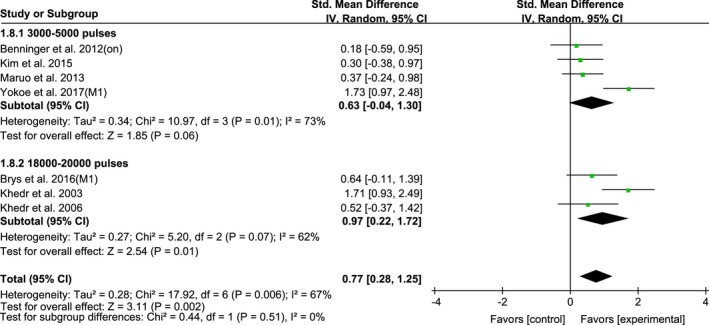
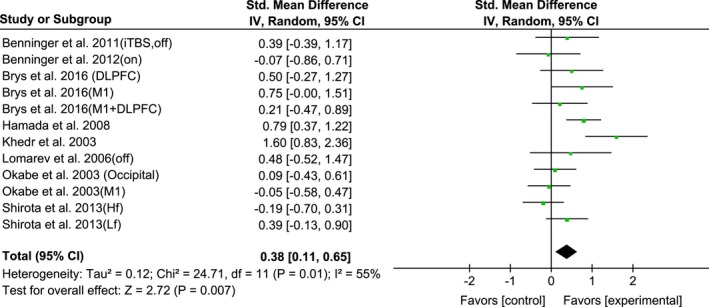
Results: Twenty-three studies with a total of 646 participants were included. The pooled estimates of rTMS revealed significant short-term (SMD, 0.37; p < 0.00001) and long-term (SMD, 0.39; p = 0.005) effects on motor function improvement of PD. Subgroup analysis observed that high-frequency rTMS (HF-rTMS) was significant in improving motor function (SMD, 0.48; p < 0.00001), but low-frequency rTMS (LF-rTMS) was not. In particular, when HF-rTMS targeted over the primary motor cortex (M1), in which the bilateral M1 revealed a larger effect size than unilateral M1. Compared to single-session, multi-session of HF-rTMS over the M1 showed significant effect size. In addition, HF-rTMS over the M1 with a total of 18,000-20,000 stimulation pulses yielded more significant effects (SMD, 0.97; p = 0.01) than other dosages.
Conclusions: In conclusion, multi-session of HF-rTMS over the M1 (especially bilateral M1) with a total of 18,000-20,000 pulses appears to be the optimal parameters for motor improvement of PD.
Keywords: Parkinson's disease; meta-analysis; motor function; repetitive transcranial magnetic stimulation.
© 2018 The Authors. Brain and Behavior published by Wiley Periodicals, Inc.
Figures
References
-
- Benninger, D. H. , Iseki, K. , Kranick, S. , Luckenbaugh, D. A. , Houdayer, E. , & Hallett, M. (2012). Controlled study of 50‐Hz repetitive transcranial magnetic stimulation for the treatment of Parkinson disease. Neurorehabilitation and Neural Repair, 26(9), 1096–1105. 10.1177/1545968312445636 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
